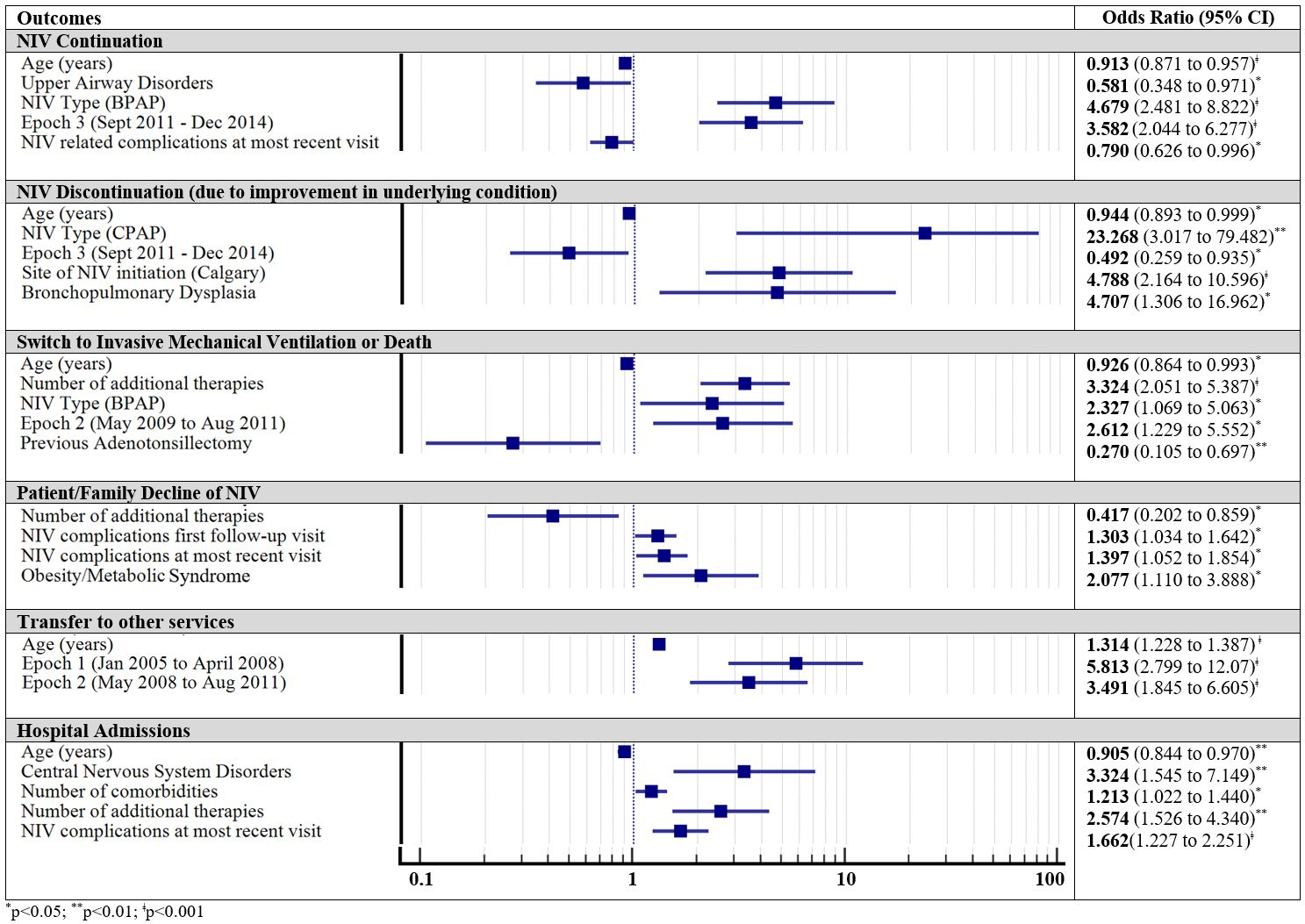
Background: Non-invasive ventilation (NIV) is a first-line therapy for sleep-related breathing disorders and chronic respiratory insufficiency. Evidence about predictors that may impact long-term NIV outcomes, however, is scarce. The aim of this study is to determine demographic, clinical, and technology-related predictors of long-term NIV outcomes. Methods: A ten-year multi-centred retrospective review of children started on long-term continuous or bilevel positive airway pressure (CPAP, BPAP) in Alberta. Demographic, technology-related, and longitudinal clinical data was collected. Long-term outcomes examined included ongoing NIV use, discontinuation due to improvement in underlying condition, switch to invasive mechanical ventilation (IMV) or death, patient/family therapy declination, transfer of services, and hospital admissions. Results: 622 children were included. Both younger age and CPAP use predicted higher likelihood for NIV discontinuation due to improvement in underlying conditions. Children with upper airway disorders or bronchopulmonary dysplasia were less likely to require NIV continuation while presence of central nervous system (CNS) disorders resulted in higher likelihood of hospitalizations and switch to IMV or death. The presence of obesity/metabolic syndrome and early NIV-associated complications predicted higher risk for NIV declination. Children with more co-morbidities or use of additional therapies required more hospitalizations and the latter also predicted higher risk to be switched to IMV or death. Conclusions: Demographic, clinical data, and NIV type impact long-term NIV outcomes and need to be considered during the initial discussions about therapy expectations with families. Knowledge of factors that may impact long-term NIV outcomes might help to better monitor at-risk patients and minimize adverse outcomes.