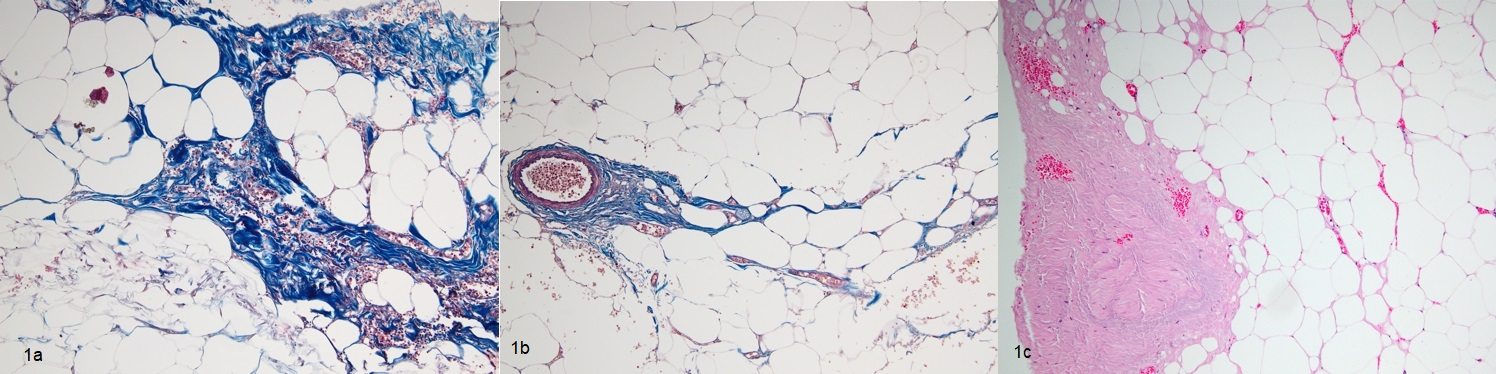
Introduction The dissection of perirenal fat is of critical importance to kidney surgery and ease of dissection is more important when using minimally invasive approaches. This study aimed to determine the clinical, radiological, and pathological significance of adherent perirenal fat(APF). Materials and Methods This prospective study included 22 patients scheduled for partial nephrectomy and 40 patients for donor nephrectomy. Intra-operative fat dissection time was recorded and the complexity of perirenal fat dissection was surgeon-classified as easy, moderate, and difficult. Perirenal fat and subcutaneous fat thickness was measured. Measurement of perirenal fat depth, and the Hounsfield unit(HU) for both perirenal and subcutaneous fields was performed using CT images. All specimens were submitted for histopatological analysis. Researchers in each arm were blinded to other researchers’ data. Results Mean age of the patients was 51.3±12.7years. Mean perirenal fat dissection time was 15.0±13.5min. Patient demographics, BMI, nor occupational status differed between the 3 complexity of perirenal fat dissection groups. Radiological findings showed that there was a significant correlation between perirenal fat depth and complexity of perirenal fat dissection(p<0.05), but not with HU measurements or subcutaneous fat thickness. Surgeon classification of the complexity of perirenal fat dissection was in accordance with the duration of dissection(p<0.05). Perinephric fat contained more fibrous tissue in the patients with histologically proven APF than in those without(p<0.05). Conclusions APF is a challenge during kidney surgery. Difficult dissection prolongs the duration of surgery, which can lead to complications. Perirenal fat thickness measured via pre-operative CT might be used to predict APF.