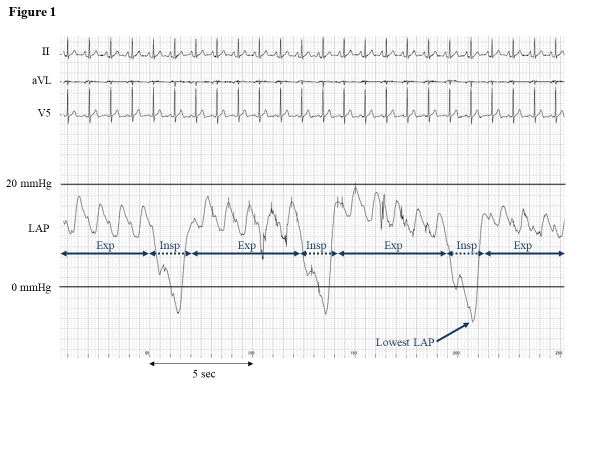
Introduction Sedation during pulmonary vein isolation (PVI) of atrial fibrillation often provokes a decline in left atrial (LA) pressure (LAP) under atmospheric pressure and increases the risk of systemic air embolisms. This study aimed to investigate the efficacy of adaptive servo-ventilation (ASV) on the LAP in sedated patients. Methods and Results Fifty-one consecutive patients undergoing cryoballoon PVI were enrolled. All patients underwent sedation using propofol throughout the procedure. Sedation status was monitored by the bispectral index. After the transseptal puncture and inserting the long sheath into the LA, the LAP was measured via the sheath. Then, the ASV treatment was started, and the LAP was re-measured. The LAP before and after the ASV support was investigated. Before the ASV, the LAP during inspiratory phase was significantly smaller than that during expiratory phase (4.9±5.4 mmHg vs. 14.0±5.2 mmHg, p<0.01). The lowest LAP was -2.2±5.1 mmHg and was under 0 mmHg in 37 (73%) patients. After the ASV, the LAP during inspiratory phase significantly increased to 8.9±4.1 mmHg (p<0.01), and lowest LAP to 4.7±5.9 mmHg (p<0.01). The negative lowest LAP value became positive in 30/37(81%) patients. There were no statistical differences regarding obstructive sleep apnea (OSA), obesity, gender, or other comorbidities between patients with and without a negative lowest LAP after the ASV support. Conclusion ASV is effective for increasing the LAP above 0 mmHg and might prevent air embolisms during PVI. A negative LAP after the ASV was rare but occurred in patients even without comorbidities such as OSA and obesity