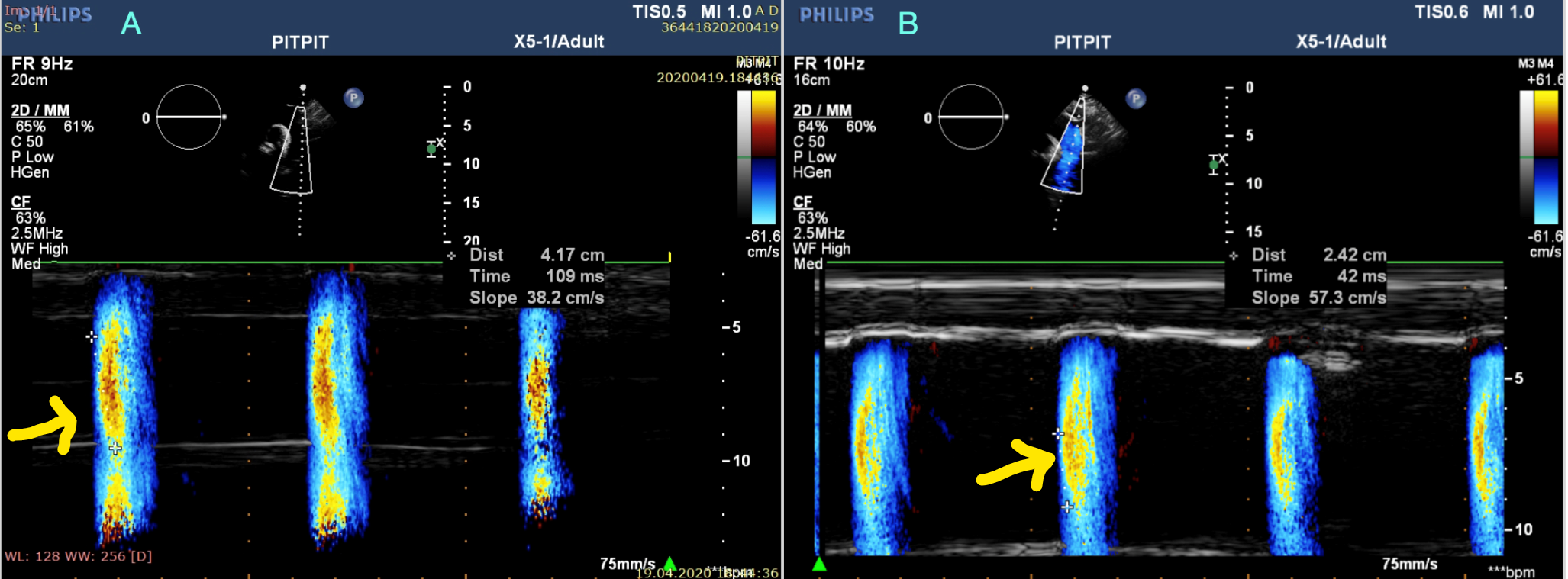
Background: Cardiovascular disease (CVD) is the primary cause of mortality and morbidity in chronic kidney disease (CKD) patients. Aortic propagation velocity (APV), epicardial fat thickness (EFT), and carotid intima-media thickness (CIMT) measurements could provide additional information on assessing renal decline in CKD patients. The study aimed to evaluate EFT, AVP, and CIMT in CKD patients and then investigate the association among those parameters. Methods and Results: A total of 170 CKD consecutive subjects were enrolled in the study. Patients were divided into five groups according to their GFR values. Each patient underwent complete transthoracic echocardiography examination. APV, EFT and CIMT were measured for analyses. A multivariate linear regression model was used for analysis to determine the independent predictors of GFR. The lowest APV was observed in stage IV-V, and the highest APV was observed in stage I-II (p<0.001). Stage IV-V patients had the highest EFT, and stage I-II patients had the lowest EFT (p<0.001). Moreover, the lowest CIMT was observed in stage III, and the highest APV was observed in stage V (p<0.001). GFR was significantly and positively correlated with APV and negatively correlated with EFT and CIMT. In multivariate analyses, APV (OR: 0.289, p<0.001), EFT (OR: -0.135, p<0.001) and CIMT (OR: -0.388, p<0.001) were independent predictors of GFR. Conclusion: We found that APV decreased, and EFT and CIMT increased as CKD progress. The present study suggests that APV, EFT, and CIMT might be incorporated with the examination of CKD patients in daily practice.