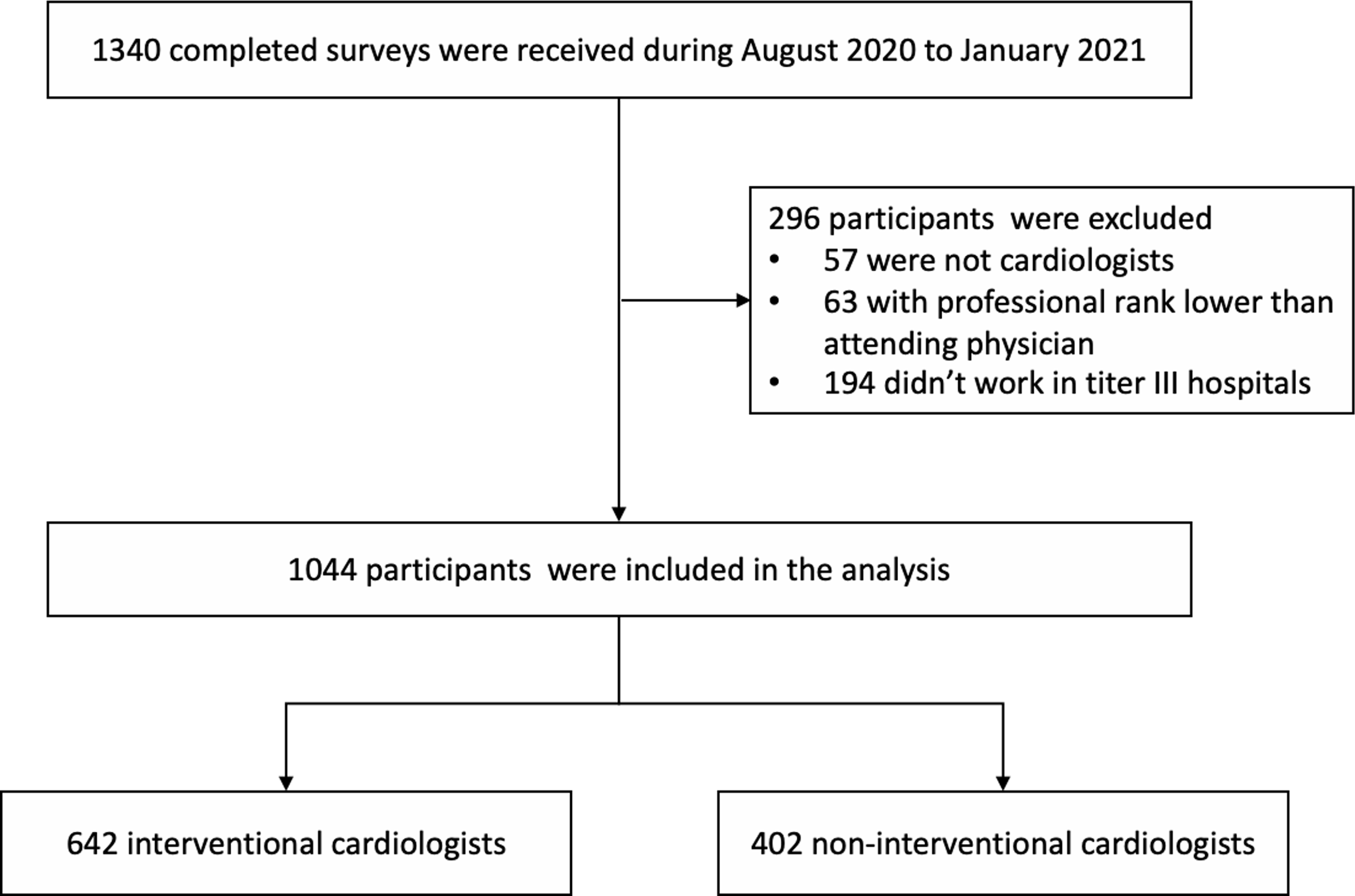
Introduction: Interventional cardiology procedures (ICPs) have become the mainstay treatments in cardiology diseases and increased rapidly. This study aims to assess the occupational health hazards (OHHs) related to the long-time wearing of lead personal protective equipment and reveal health protection needs in interventional cardiologists. Methods and Results: We invited interventional and non-interventional cardiologists in tertiary III hospitals in China to participate in an online cross-sectional survey on their health status, utilization of personal protective equipment (PPE), and personal health protection (PHP) needs. Propensity score methods were used for comparisons of OHHs between the matched interventional and non-interventional cardiologists. Totally, 642 interventional and 402 non-interventional cardiologists completed the survey. The interventional cardiologists had significantly higher incidence of body pain (56.6% vs. 24.2%, p<0.001), bone and joint disease (21.7% vs. 8.6%, p=0.001), cataract (3.5% vs. 0%, p=0.039), and anxiety (8.1% vs. 2.5%, p=0.029) than the matched non-interventional cardiologists. The risk of back pain was independently associated with female gender, performing percutaneous coronary intervention procedure or ≥2 types of ICP, and the personal annual volume of ICPs. Only 3.3% of interventional cardiologists were satisfied with PPE and 83.0% of them complained of physical toll caused by heavy PPE. 90.7% were willing to conduct ICP without radiation exposure. Conclusions: Body pain was the main OHH in interventional cardiologists likely due to wearing heavy lead PPE for long working hours. Besides training more interventional cardiologists, the adoption of emerging technologies without heavy lead PPE will be a promising way to reduce the OHH burden.