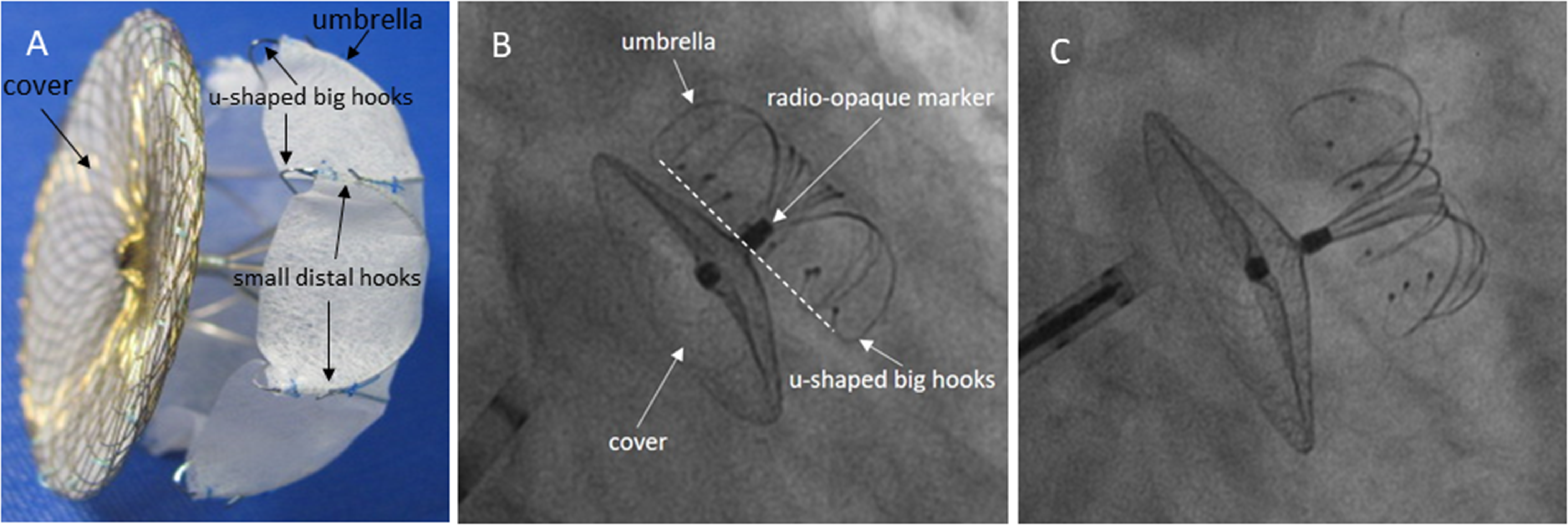
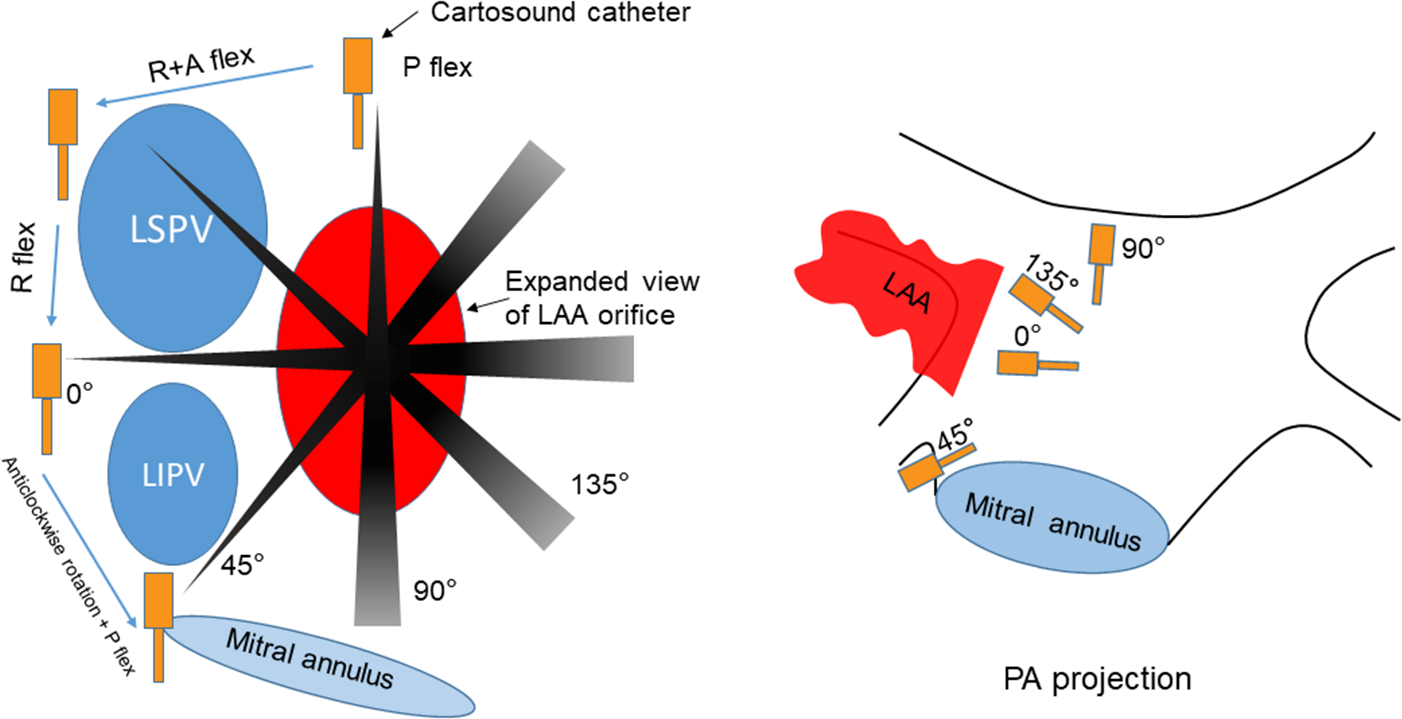
Introduction: Transesophageal echocardiography (TEE) fails to display optimal views to guide left atrial appendage closure (LAAC) procedure in some patients due to atrio-esophageal anatomical limitation. We aimed to investigate if intracardiac echocardiography (ICE) conducted from left atrium (LA) achieves comparable multi-planar views and clinical outcomes as TEE during LAAC. Methods and Results: This study prospectively enrolled 102 consecutive patients with non-valvular atrial fibrillation receiving LAmbre implants under local anesthesia at the First Affiliated Hospital of Wenzhou Medical University from August 2018 to July 2019. The procedures were guided by either ICE (n=40), TEE (n=50) or combined ICE-TEE (n=12). A novel multi-angled “FLAVOR” approach was used in ICE group for assessment. ICE allowed visualization of implanted device in all patients at all proposed angles with long-axis views, while TEE failed to do so in at least one of the angles in 36% of cases. In the combined ICE-TEE cohort, TEE failed peri-device leak assessment in 2 patients. Rates of procedural success, recapture, resizing and complications were similar between ICE and TEE groups. Fluoroscopy time, radiation dose and volume of contrast use in ICE group were significantly lower than the TEE cohort. At 45-day TEE follow-up, rate and degree of peri-device leaks were similar between the ICE and TEE groups. Conclusions: A systematic approach using ICE to guide LAmbre LAA occlusion was safe and feasible. This method was more reliable in comprehensive, multi-angled imaging assessment, and achieving shorter fluoroscopy time, lower radiation dose and less contrast use than TEE.