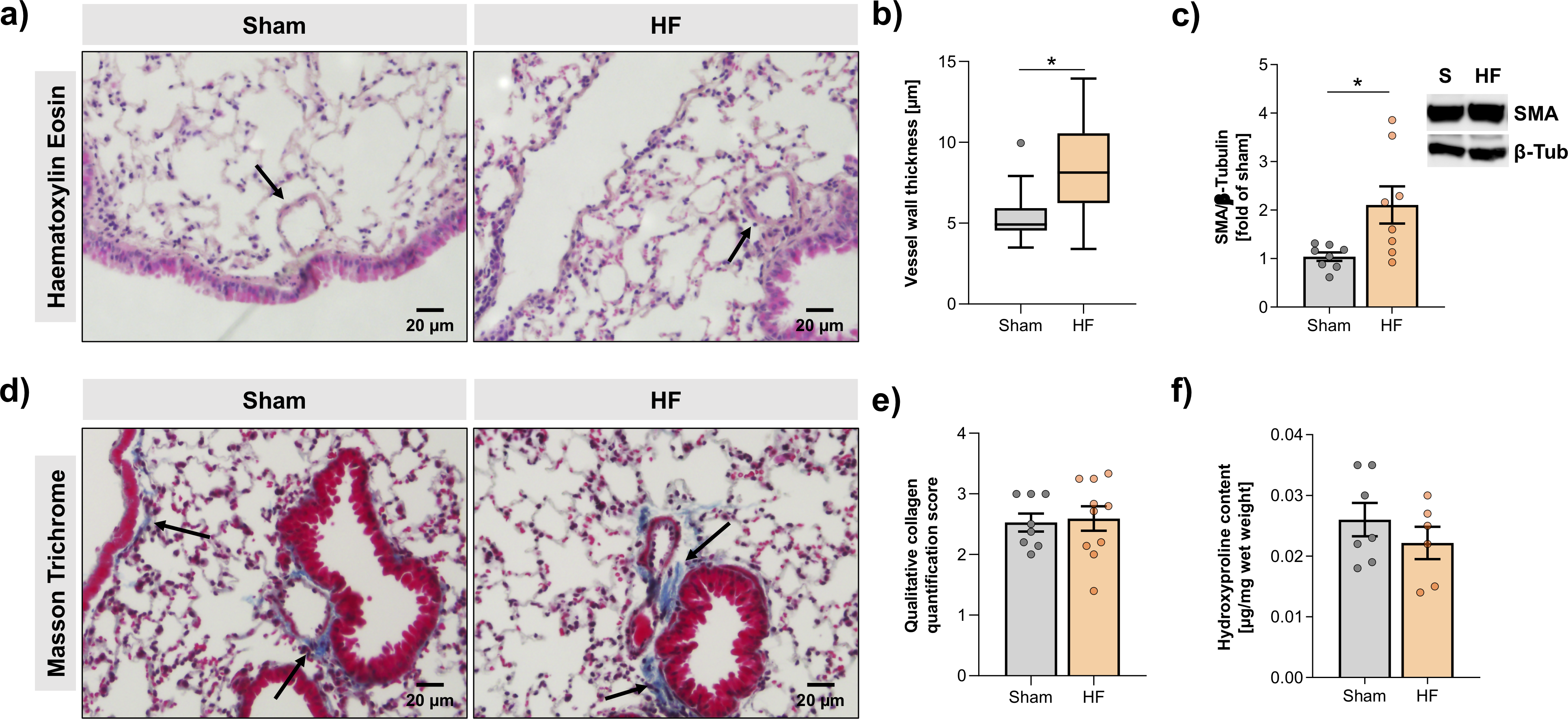
Aims:Heart failure (HF) affects 64 million people worldwide. Despite advancements in prevention and therapy, quality of life remains poor for many HF patients due to associated target organ damage. Pulmonary manifestations of HF are well-established. However, difficulties in the treatment of HF patients with chronic lung phenotypes remain, as standard therapies are often complicated by contraindications. The aim of this study is to investigate thecystic fibrosis transmembrane regulator (CFTR) involvement in lung inflammation during HF, a concept that may provide new mechanism-based therapies for HF patients with pulmonary complications.Methods and Results:Ligation of the left anterior descending coronary artery in mice was used to induce myocardial infarction (MI). At 10 weeks post-MI, pharmacological CFTR corrector therapy (i.e., Lumacaftor (Lum)) was applied systemically or lung-specifically for 2 weeks, and the lungs were analysed using histology, flow cytometry, western blotting, and qPCR. Experimental HF is associated with an apparent lung phenotype characterized by vascular inflammation and remodelling, pronounced tissue inflammation as evidenced by infiltration of pro-inflammatory monocytes, and a reduction of pulmonary CFTR+ cells. Moreover, the elevation of a classically-activated phenotype of non-alveolar macrophages coincided with a cell-specific reduction of pulmonary CFTR expression. Pharmacological correction of CFTR with Lum mitigated the HF-induced downregulation of pulmonary CFTR expression, increased the proportion of CFTR+cells in the lung, and diminished the HF-associated elevation of classically-activated non-alveolar macrophages within the lungs with implication for vessel wall thickness.Conclusion:Collectively, our data suggest that downregulation of CFTR in the HF lung extends to non-alveolar macrophages with consequences for tissue inflammation and vascular structure. Pharmacological CFTR correction possesses the capacity to alleviate HF-induced inflammation in the lung and may emerge as treatment option for HF patients with chronic lung phenotypes.