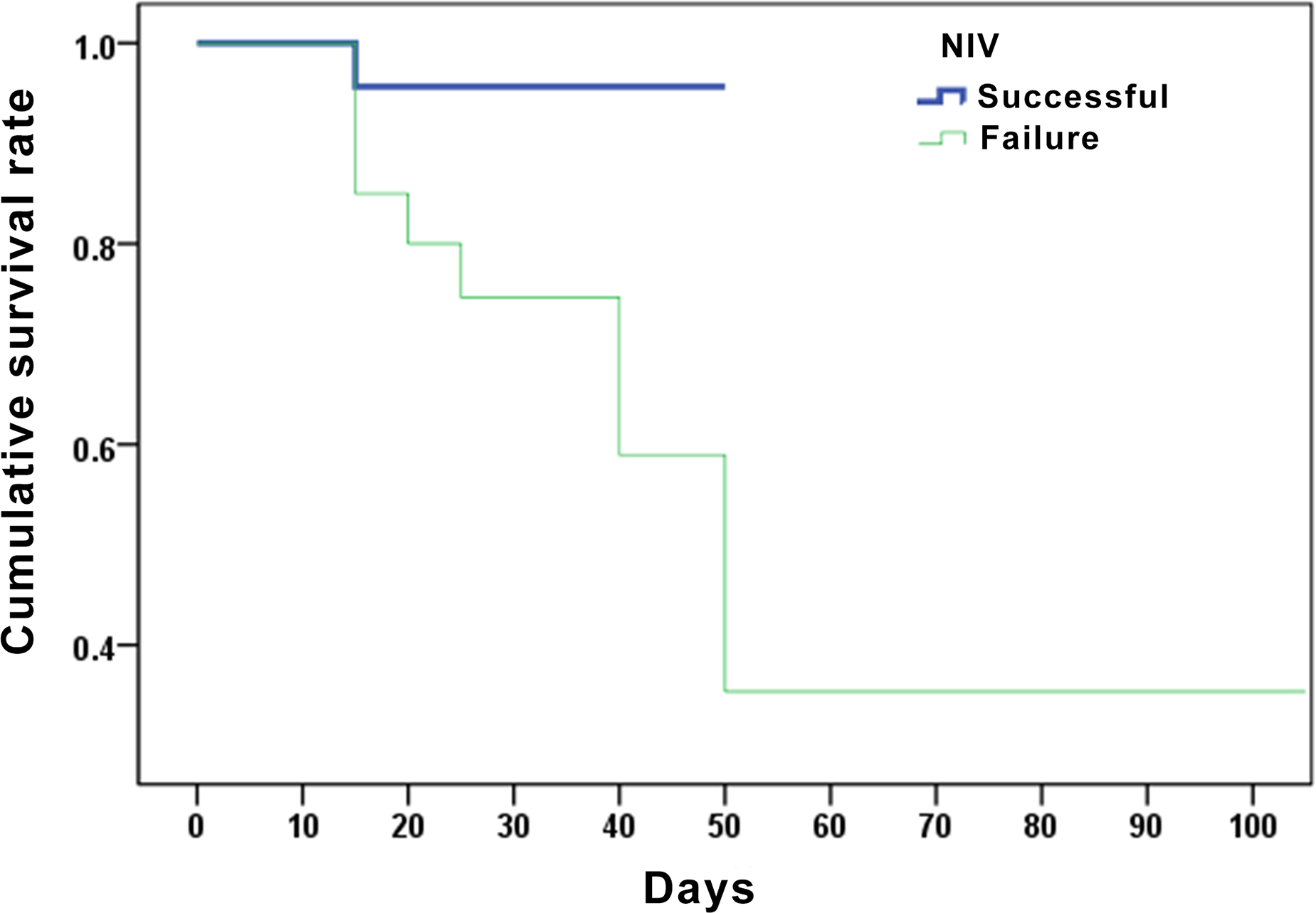
Background:The inappropriate mechanical ventilation strategy could improve the mortality rate of patients with influenza A-associated ARDS.Therefore, clinical data are needed to support the timing of NIV therapy for patients with influenza A-associated ARDS. Methods: For this retrospective cohort study, data were obtained from the Fuzhou Pulmonary Hospital of Fujian, China. Differences in baseline factors, risk factors, and outcome parameters were studied between patients with and without invasive mechanical ventilation. Results: Among this cohort, 24 patients received successful NIV with an average age of (57.96±17.08) years. NIV failure occurred in 21 patients with an average age of (54.19±14) years. Mortality data were obtained for the successful NIV group and the mortality rate was lower than in the failed NIV group [4.17%vs42.86%, X2=7.591, P = 0.003]. The independent risk factors for the success of NIV were APACHE II score and LDH (OR=1.830, 95%CI 1.105-3.032 and OR=1.011, 95% CI 1.001-1.020, respectively). When the OI is <95 mmHg, APACHE II>19 and LDH>498U/L, the sensitivity and specificity of predicting failed NIV were [66.67% (95% CI 43% - 85.4%) , 87.5% (95% CI 67.6% - 97.3%)], [85.71% (95% CI 63.7%-97%), 79.17% (95% CI 57.8%-92.9%)] and [90.48% (95% CI 69.6%-98.8%), 62.5% (95% CI 40.6%-81.2%)], respectively. Conclusions: Overall, patients with influenza A-associated ARDS receiving successful NIV have lower mortality rates than those for whom NIV failed. Independent risk factors for successful NIV are LDH and APACHE II scores.Invasive mechanical ventilation can possibly be avoided in some patients with 200 mmHg > OI > 95 mmHg.