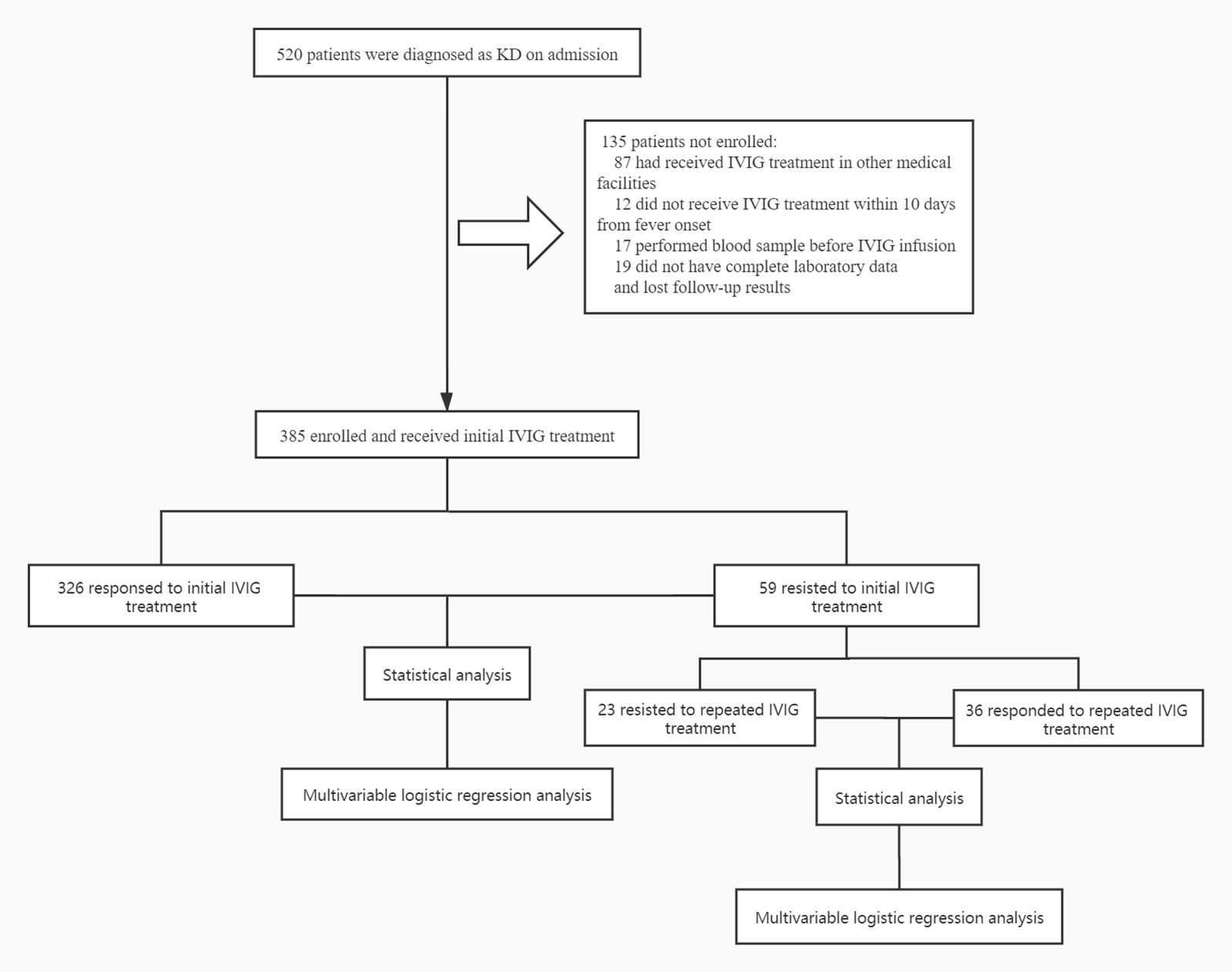
Background: Intravenous immunoglobulin (IVIG) resistance prediction remains substantial in Kawasaki disease (KD), with limited data on the predictive value of coagulation profile for IVIG resistance, particularly for repeated IVIG resistance. Therefore, the aim of our study was to testify the predictive validity of coagulation profile for both initial and repeated IVIG resistance in KD. Methods: A total of 385 KD patients were prospectively recruited between April in 2015 and May in 2019. Coagulation and other profiles were evaluated between IVIG-responsive and IVIG-resistant groups. Multivariate logistic regression analysis was applied to determine the association between coagulation profiles and IVIG resistance. ROC curves analysis was further performed to assess validity of coagulation profiles in predicting both initial and repeated IVIG resistance. Results: PT, APTT and D-dimer were significantly increased in initial IVIG-resistant group with ATIII significantly reduced. Meanwhile, ATIII was declined markedly in repeated IVIG-resistant patients. PT, APTT, D-dimer and ATIII cutoff values of 13.95 s, 41.15 s, 1.48 mg/l, and 89.5% yielded sensitivities of 73%, 32%, 71%, 81%; specificities of 55%, 88%, 62%, 51% for predicting initial IVIG resistance, respectively. The cutoff value of ATIII for predicting repeated IVIG resistance was 68.5%, with sensitivity of 71% and specificity of 55%. Multivariate logistic regression analysis showed that PT, APTT, D-dimer and ATIII were independent risk factors for initial IVIG resistant patients with KD. Conclusions: Coagulation profiles were significantly dysregulated in KD patients. Some of them particularly ATIII may serve as complementary laboratory markers for prediction of both initial and repeated IVIG resistance.