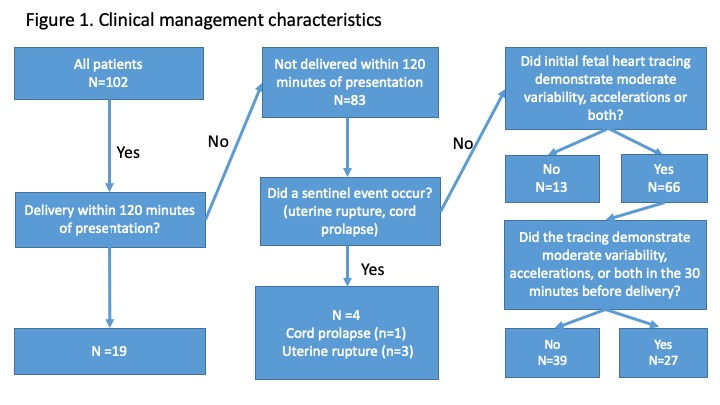
OBJECTIVE: To characterize clinical management of deliveries resulting in neonatal hypoxic ischemic encephalopathy. DESIGN: Retrospective case series SETTING: Three academic referral medical centers in the United States POPULATION: All neonates ≥35 weeks’ gestation with HIE based on cord blood pH<7.0, base deficit of ≥12.0mmol/L, along with relevant radiological, laboratory, and clinical findings. METHODS: Clinical management was characterized based on whether (i)delivery occurred within 120 minutes of presentation, (ii)delivery occurred due to a sentinel event such as cord prolapse or uterine rupture, and (iii)the fetal heart rate tracing(FHR) demonstrated variability, accelerations, or both upon presentation and in the half hour before delivery. MAIN OUTCOME MEASURES: Relationship of mode of delivery to FHR tracing characteristics at delivery. Obstetric outcomes, labour course and management were analysed. RESULTS: Of 144,904 deliveries, 102 maternal-newborn dyads met criteria. Of these, 19 delivered within 120 of minutes of presentation and four further women experienced a sentinel event. Of the remaining 79, 66(84%) had a FHR tracing on presentation that demonstrated variability, accelerations or both. Of these 66 cases, 27 had a fetal heart tracing that demonstrated variability, accelerations or both in the 30 minutes preceding delivery. CONCLUSION: Approximately two-thirds of cases of HIE occurred in cases where the FHR tracing initially demonstrated variability, accelerations, or both, without a sentinel event and without a condition requiring delivery within 120 minutes of presentation. Of these >40% had variability, accelerations, or both in the half hour before delivery. This suggests additional insights are required to prevent some cases of HIE.