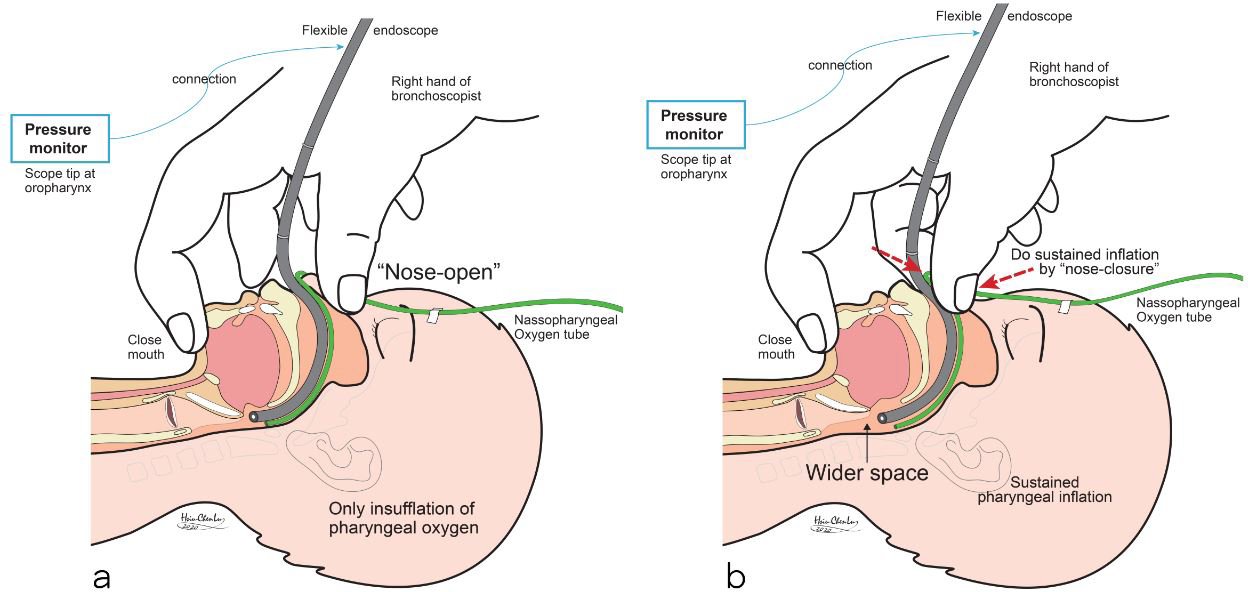
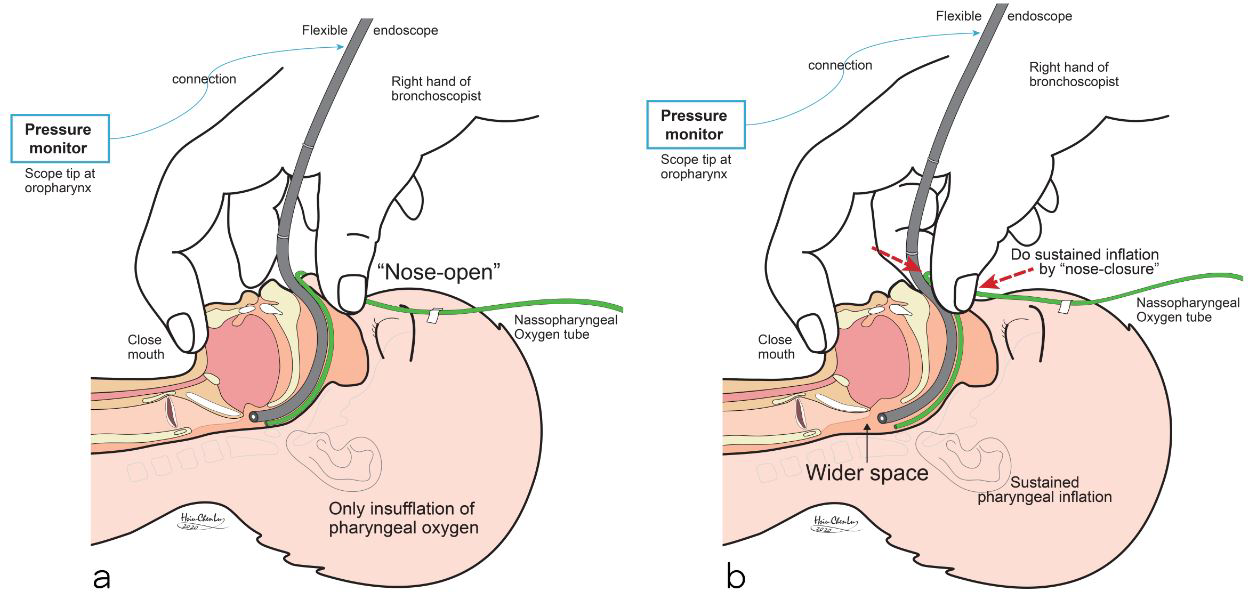
Sustained pharyngeal inflation (SPI) with pharyngeal oxygen and nose-close (PhO2-NC) can create positive inflation pressure (PIP) inside the pharyngolaryngeal space (PLS). This study measured and compared effects of different SPI durations in the PLS. Method: A one-year prospective study, 20 consequent infants whose age less than 3-year-old and scheduled for elective FB were enrolled. SPI performed in four different durations (0.0, 1.0, 3.0 and 5.0 seconds) consequently. Each infant did two cycles of SPI. Measured the PIP of each SPI in the pharynx, and simultaneously took images at three locations of oropharynx, supra-larynx and larynx. Data of infant’s demographics, PIP levels, space expansion scores and images were collected and analyzed. Results: Total 20 studied infants, the mean (SD) age was 11.6 (9.1) month-old, the mean (SD) body weight was 6. 8 (2.4) kg and the mean (SD) study time was 3.8 (1.1) minutes. The measured mean (SD) pharyngeal PIPs were 4.1 (3.3), 21.9 (7.0), 42.2 (12.3) and 65.5 (18.5) cmH2O at SPI duration of 0.0, 1.0, 3.0 and 5.0 seconds, respectively. Which showed positively and significantly (p<0.001) correlations. At these assigned locations, the corresponding PLS images also show significant lumen expansion correlated with the PIP. Especially, when there existed pathologic or occult lesions. No any study related complication was noted. Conclusions: SPI with PhO2-NC up to 5 seconds is a simple, safe and feasible clinical ventilation modality. Which could provide enough PIP to expand the PLS and benefit FB performance in infants.