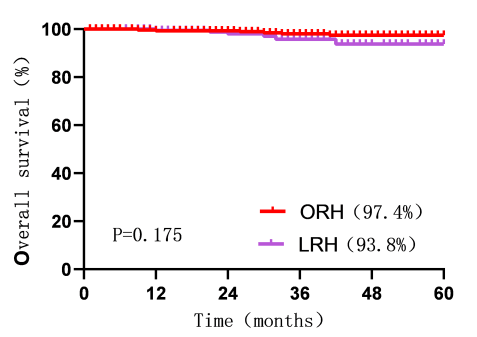
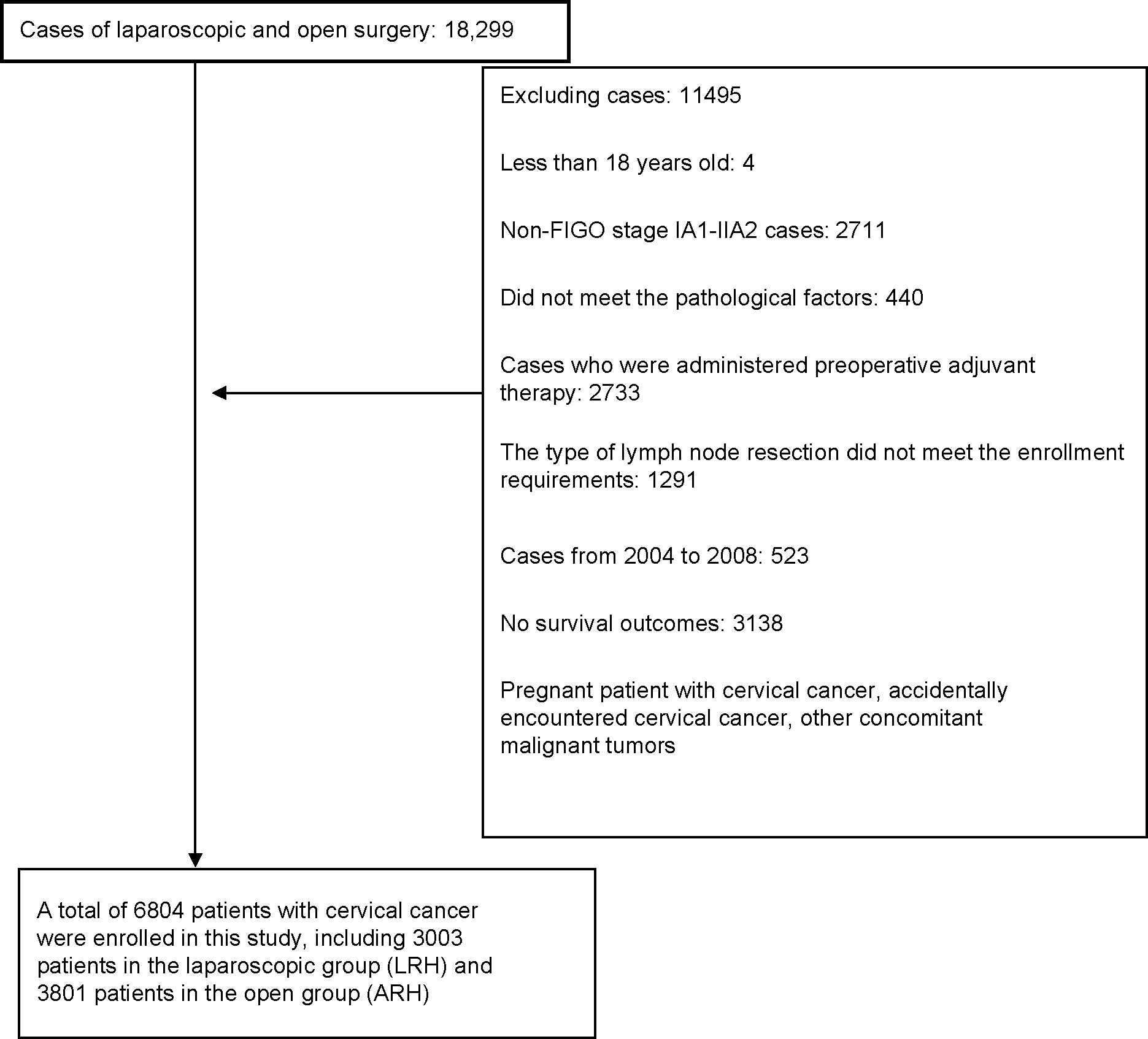
Objective: Compare the outcomes associated with laparoscopic radical hysterectomy (LRH) and abdominal radical hysterectomy (ARH) for cervical cancer. Design: Retrospective, multicenter observational analysis Setting: Select patients of LRH and ARH from cervical cancer database and compare their outcomes. Population: Patients with stage IA1 (Lymphovascular space invasion [LVSI]-positive) and stage IIA2 cervical cancer (N=6804) were enrolled, of whom 3003 underwent laparoscopy (LRH group), and 3801 underwent laparotomy (ARH group). Methods: Kaplan-Meier survival analysis,propensity score matching (PSM) and Cox regression. Main Outcome Measures: Five-year overall survival (OS) and 5-year disease-free survival (DFS) Results: Before PSM, there was no difference in outcomes between the groups (5-year OS: LRH 89.2% vs. ARH 90.6%, P=0.903.; 5-year DFS: LRH 84.5% vs. ARH 87.1%, P=0.155). Surgical approach did not affect 5-year OS; however, it did affect 5-year DFS (hazard ratio [HR]=0.827, 95% confidence interval [CI]: 0.711-0.962, P=0.014). After PSM, there was no difference in 5-year OS between the LRH (N=1828) and ARH (N=1828) groups (91.0% vs. 93.1%, P=0.220); but there was a significant difference in 5-year DFS between the LRG and ARH groups (86.2% vs. 90.6%, P=0.002). Cox regression revealed that the surgical approach did not affect 5-year OS; however, it did affect 5-year DFS (HR=0.701, 95% CI: 0.563-0.874, P=0.002). Conclusions: For IA1 (LVSI-positive) and IIA1 cervical cancers, the recurrence rate following laparoscopic surgery was higher than that following open surgery, regardless of the surgeon’s experience.