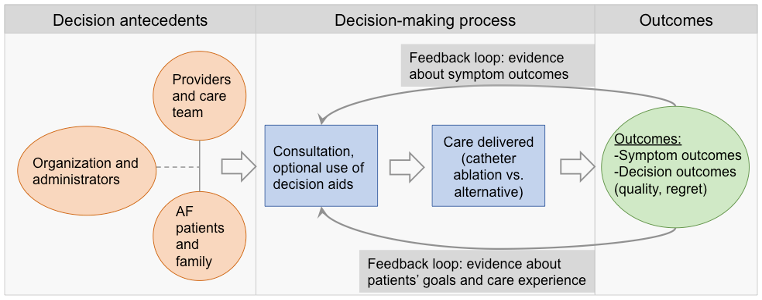
Introduction: Shared decision-making (SDM) can support patients with atrial fibrillation (AF) to evaluate treatment options for rhythm and symptom control, but studies suggest it is not occurring meaningfully in routine practice. The objective of this study was to measure decision quality and describe decision-making processes among patients and clinicians involved in decision-making around catheter ablation for AF. Methods: We conducted a cross-sectional, mixed-methods study guided by a SDM model outlining decision antecedents, processes, and outcomes. Patients and clinicians completed semi-structured interviews about decision-making around ablation, feelings of decision conflict and regret, and preferences for the content, delivery, and format of a hypothetical decision aid for ablation. Patients also completed surveys about demographic characteristics and literacy levels, AF symptoms using the University of Toronto AF Severity Scale (AFSS), and aspects of decision quality using the Controls-Preferences, Decisional Conflict, and Decision Regret scales. Surveys were analyzed using descriptive statistics and qualitative data were analyzed using directed content analysis. Results: Fifteen patients (mean age 71.1 ± 8.6 years; 27% female; mean 7.0 [SD 7.0] months since ablation) and five clinicians (three physicians, one NP, and one PA) were recruited. Most patients preferred to either share or relinquish control in medical decision-making to clinicians. For most patients, decisional conflict and regret were low, and symptoms and cardiac health generally improved after ablation. However, they also reported low levels of information and agency in the decision-making process. Most clinicians report routinely providing patients with information and encouraging engagement during consultations. Patients reported preferences for an interactive, web-based decision aid that clearly presents evidence regarding outcomes using data, visualizations, videos, and personalized risk assessments, and is available in multiple languages. Conclusions: Disconnects between clinician efforts to provide information and bolster agency and patient experiences of decision-making suggest decision aids may be needed to improve decision quality in practice. Reported experiences with current decision-making practices and preferences for decision aid content, format, and delivery can support the user-centered design and development of a decision aid.