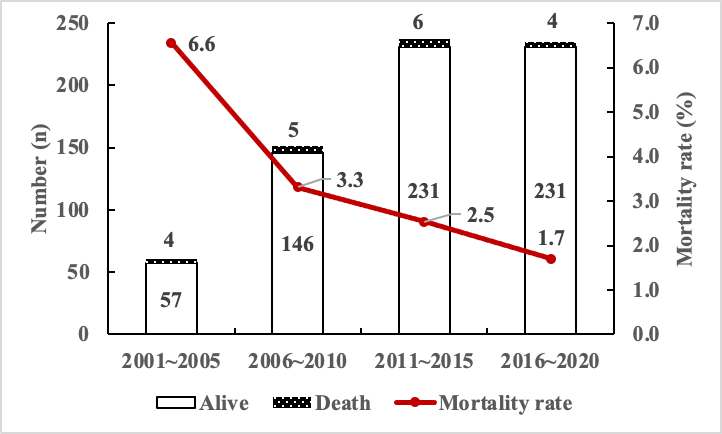
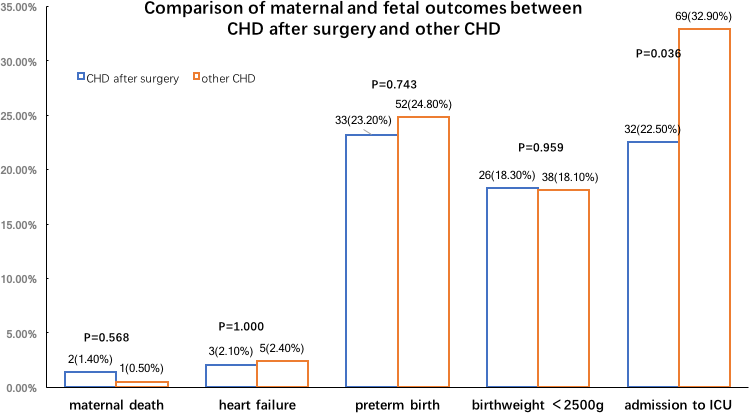
In this study, we aim to find out maternal and fetal outcomes in women with PH resulting from different causes and try to determine the risk factors related to adverse maternal and fetal outcomes. We extracted the data from the records: the demographic information, onset, course, clinical and echocardiographic details, maternal and fetal complications, management as well as obstetric data, which included complications, infant of low-birth weight. We compared the outcome based on the cause of disease and pulmonary hypertension pressure levels. 603 women were included in the final analysis, who were mainly had pulmonary hypertension secondary to congenital heart disease (66.0%) and 46 of whom had Eisenmenger syndrome (7.6%). The mortality was 3.0%, 56% of which was caused by Eisenmenger syndrome. The abortion rate was 8.3% and 32% of live newborns were born before term. Heart failure complicated 17.1% and fetal growth restriction 3.5% of pregnancies. Advanced medication was administered in an increasing number of patients. Morbidity was significantly increased in women with pulmonary hypertension associated with a pulmonary hypertension pressure ≥80 mmHg. The mortality rate was lower than previously reported. Nevertheless, in Eisenmenger syndrome, PH secondary to connective tissue disease and idiopathic PH, the maternal mortality is still very high. In addition to the use of PAH-targeted drugs, we believe that standardized maternal management strategies can also help reduce mortality, including screening for heart disease and effective transport of critically ill patients. The maternal and infant outcome is related to etiology and the severity of PASP.