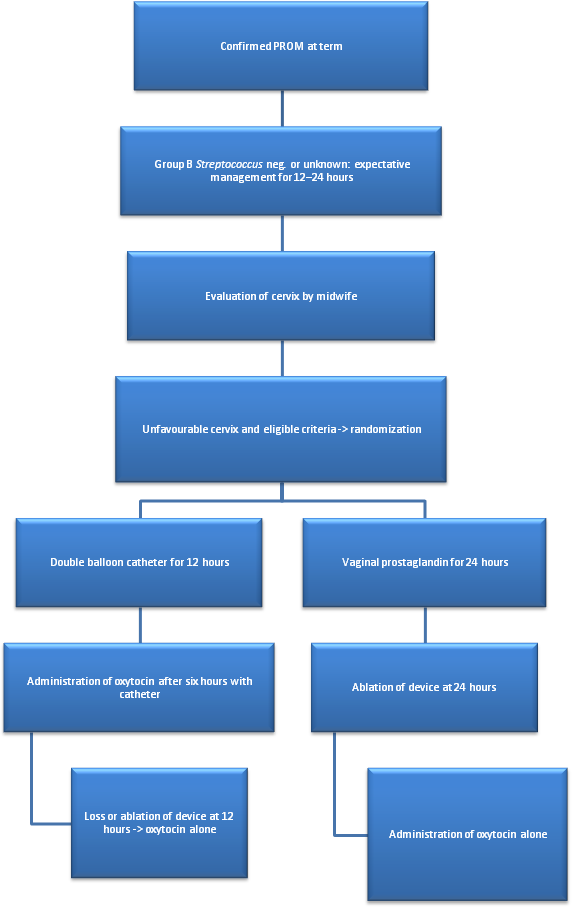
Objective: To demonstrate that a double balloon catheter combined with oxytocin decreases time between induction of labour and delivery (TID) as compared to a vaginal dinoprostone insert in cases of PROM at term. Design: Prospective, randomized, controlled trial. Setting: French university hospital Population: Patients undergoing labour induction for PROM at term with unfavorable cervix. Methods: We compared the double balloon catheter over a period of 12 hours with adjunction of oxytocin 6 hours after catheter insertion, versus dinoprostone vaginal insert. After device ablation, cervical ripening continued only with oxytocin. Main outcome measures: The primary outcome was TID. Secondary outcomes concerned delivery mode, maternal and fetal outcome and were adjusted for parity. Results: 40 patients per group were randomized. Each group had similar baseline characteristics. The study failed to demonstrate reduced TID (16.2 vs 20.2 hours, ES = 0.16 (-0.27 to 0.60), p=0.12) in catheter group versus dinoprostone except in nulliparous women (17.0 vs 26.5 hours, ES = 0.62 (0.10 to 1.14), p=0.006). The rate of vaginal delivery <24h significantly increased with combined induction (88.5% vs 66.6%, p=0.03). No statistical difference was observed concerning caesarean rate (12.5% vs 17.5%, p>0.05), chorioamnionitis (0% vs 2.5%, p=1), postpartum endometritis, maternal or neonatal outcomes. Procedure-related pain and tolerance to devices were found to be similar for the two methods. Conclusion: The double balloon catheter combined with oxytocin is an alternative for cervical ripening in case of PROM at term, and may reduce TID in nulliparous women.