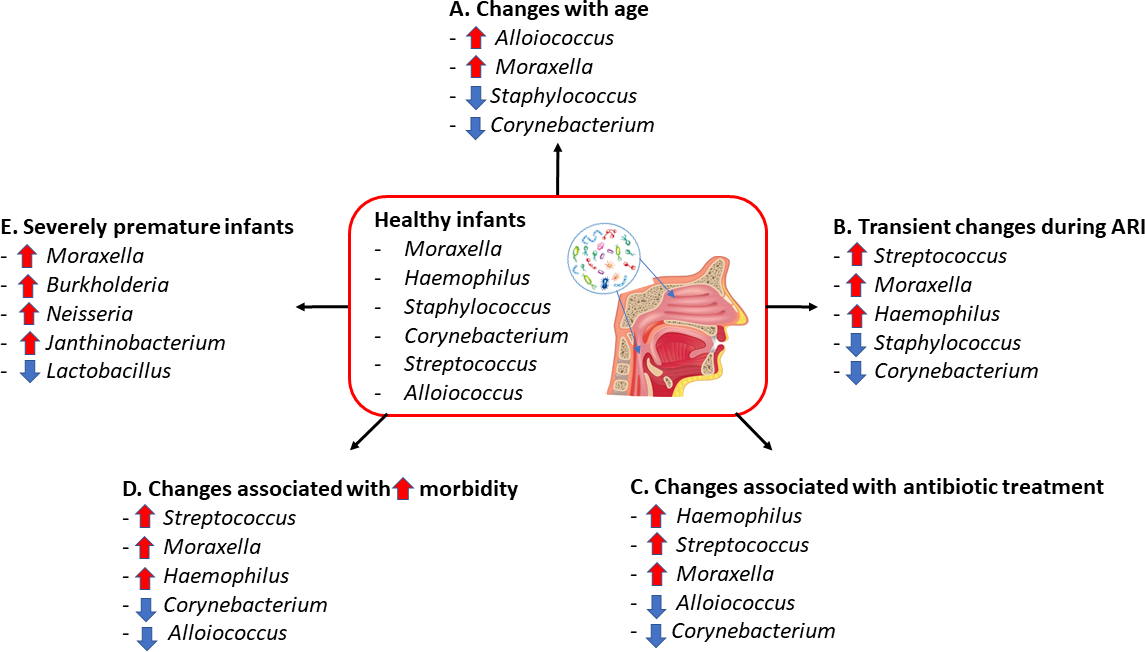
The immunopathology of respiratory syncytial virus (RSV) infection, the most common cause of lower respiratory tract infections (LRTI) in the pediatric population, with severe disease being the exception. The variability of the clinical presentation is incompletely explained by host, viral and environmental factors but, in infants and young children, disease severity is certainly linked to the physiological immune immaturity. There is evidence that the maturation of the host immune response is, at least in part, promoted by the composition of the nasopharyngeal microbiome that, modulating excessive inflammation, can counteract the predisposition to develop viral respiratory infections and lower the risk of disease severity. However, interaction between the nasopharyngeal microbiota and respiratory viruses can be bidirectional. Microbial dysbiosis can drive disease pathogenesis but may also represents a reflection of the disease-induced alterations of the local milieu. Moreover, viruses like RSV, can also increase the virulence of potential pathogens in nasopharynx, which is a main reservoir of bacteria, and therefore promote their spread to the lower airways causing superinfection. Negative changes in microbial community composition in early life may constitute a heightened risk towards severe RSV respiratory infection and bacterial superinfection, whilst specific groups of microorganisms can be associated with protection. A better understanding into the potential negative and positive role of the different nasopharyngeal bacterial species in disease prevention as well as into the possible benefits of microbiome therapeutic manipulation, may improve patient outcomes.