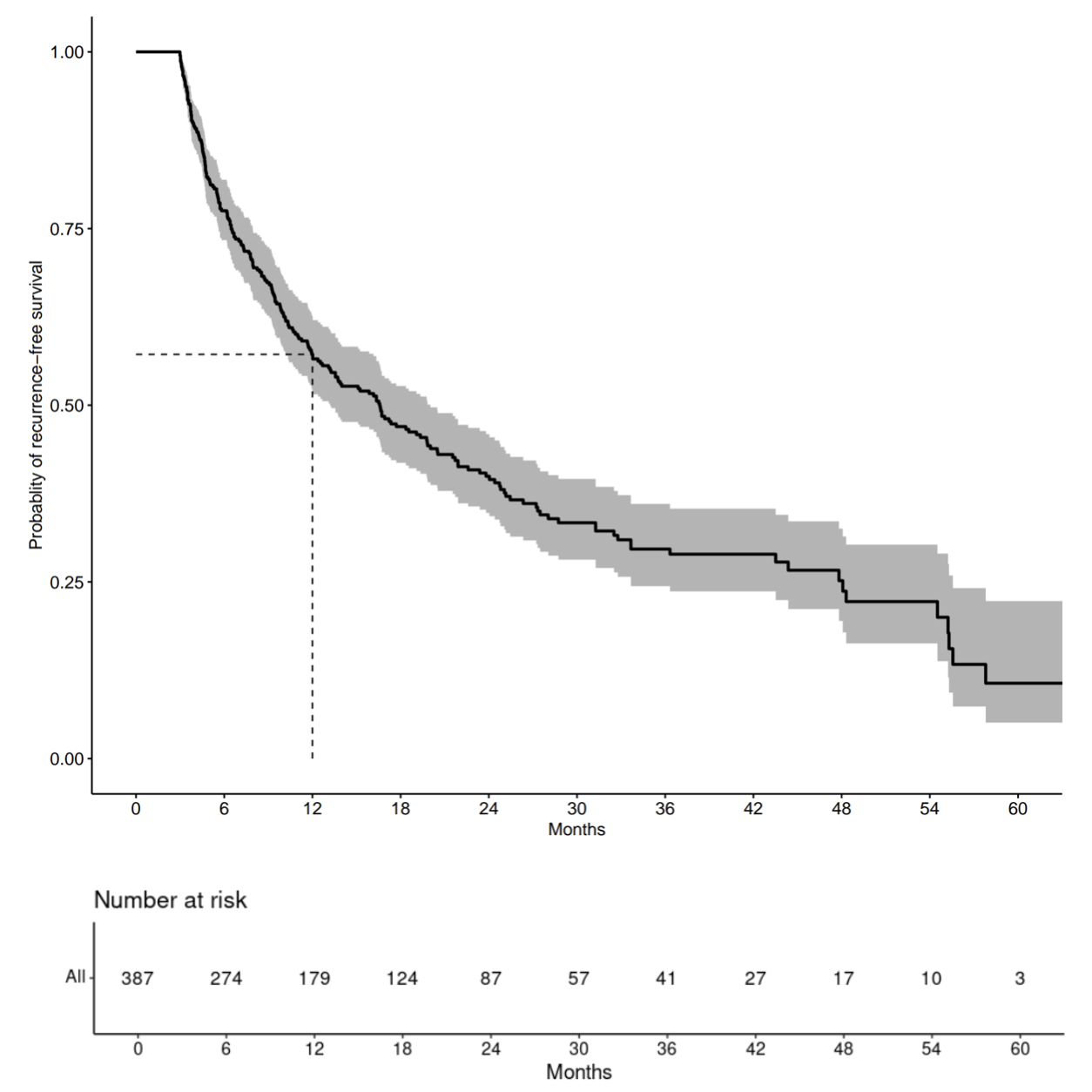
Background: Atypical Atrial Flutter (AAFL) prevalence is increasing due to the escalating Atrial Fibrillation (AF) ablations and cardiac surgeries. We wanted to explore the outcome of the AAFL ablation, considering the recent changes in mapping and ablation. Methods: This study was approved by the Institutional Review Board (IRB) of Mayo Clinic hospital. We retrospectively studied 419 patients who had undergone AAFL ablation at Mayo Clinic from January 2017 to June 2022. Thirteen patients declined research authorization, and 19 patients were lost to follow-up during the 90-day blanking period, resulting in a sample size of 387. The median follow-up time for patients was 25.7 months (95% CI 23.7, 32.3). Results: Recurrent symptoms with documentation of atrial arrhythmia Occurred in 226/387 (58.4%) patients, of which 151/226 (66.8%) occurred within the first year. The median time to recurrence was 8.5 months (max 57.8 months). Eleven patients died during the study period, 9 of whom experienced recurrence prior to death. Overall, the median recurrence-free survival (RFS) time was 16.6 months (95% CI 13.2, 20.0) with a 1-year RFS rate of 57.2% (95% CI 52.2, 62.7%). Acute termination occurred 324/387 (83.7%) during the ablation. The 1-year RFS rate was 58.9% (95% CI 53.5%, 64.9%) for patients with acute termination and 49.0% (95% CI 37.9%, 63.4%) for those without acute termination. The rate was not significantly different based on acute termination status (p = 0.11). Conclusions: The one-year RFS rate of 57.2% following AAFL ablation, even though 83.7% achieved acute termination during the procedure, signifies the extent of the underlying substrate abnormalities.