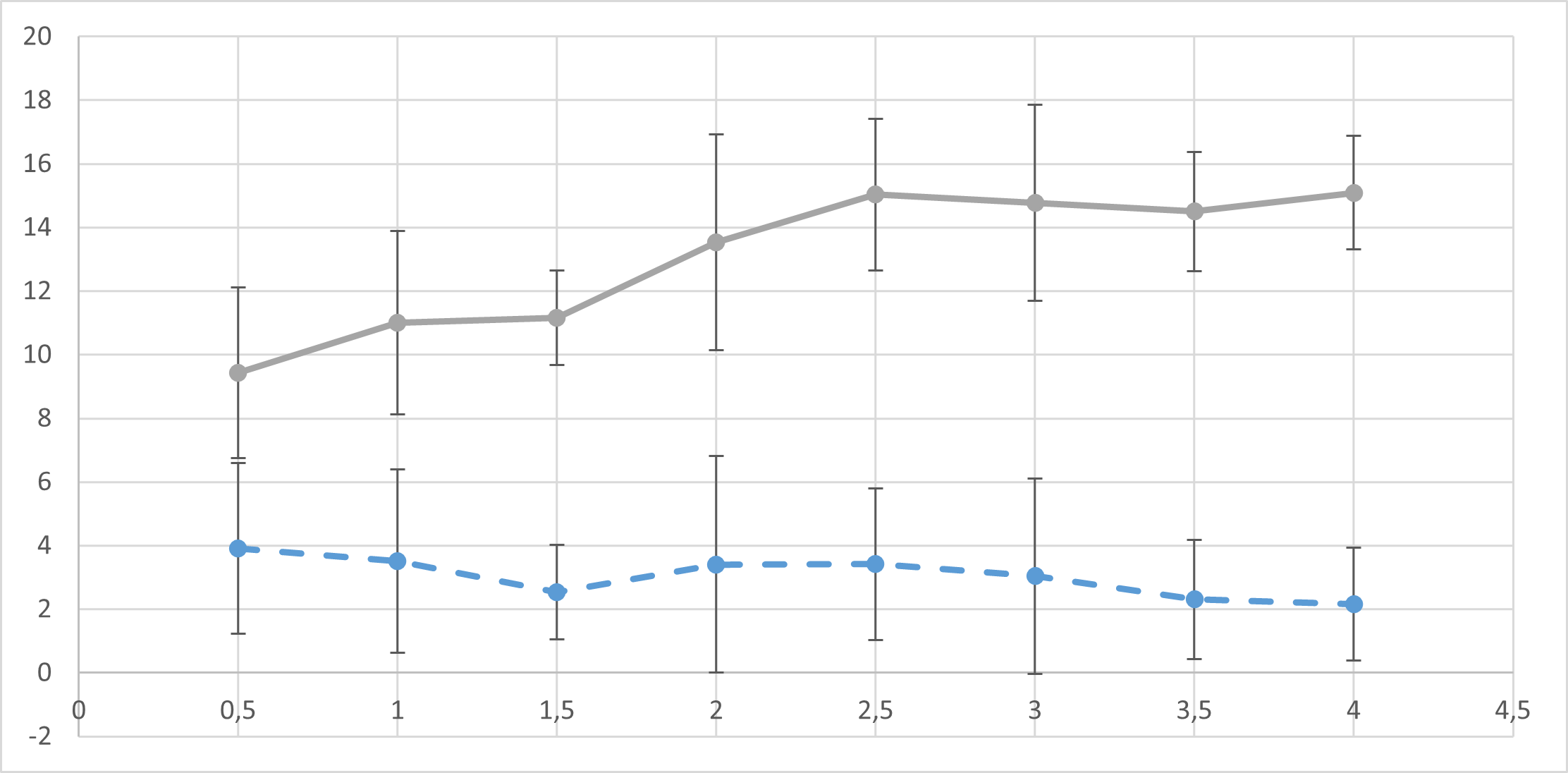
Objective: to examine the effect of changing levels of support (NAVA-level) during neurally adjusted ventilatory assist (NAVA) in preterm infant with respiratory distress syndrome (RDS) on electrical diaphragm activity. Methods: we included preterm infants admitted to the NICU, who were clinically stable and supported with NAVA, either via an endotracheal tube or via a nasal interface. Patients were recruited in the first 24 hours after the start of NAVA. Following a predefined titration protocol, NAVA levels were progressively increased starting from a level of 0,5 cmH2O/µV and with increments of 0,5 cmH2O/µV every 3 minutes, up to a maximum level of 4,0 cmH2O/µV. Respiratory and ventilation parameters were continuously recorded. Results: Ten patients were studied on NIV-NAVA and three on invasive NAVA. The NIV-NAVA patients had an average gestational age at birth of 31,4 + 3,2 weeks and an average birth weight of 1615 + 609 g. For all patients a breakpoint could be identified during the titration study. The breakpoint was on average at a level of 2,35 + 0,63 cmH2O/µV in the NIV-NAVA group. With increasing NAVA levels, the respiratory rate decreased significantly. For the other parameters no clear trend was observed. No severe complications occurred. Conclusion: Preterm neonates with RDS supported with NAVA display a typical biphasic response to changing NAVA-levels with an identifiable breakpoint. This breakpoint was at a higher NAVA-level than commonly used in this clinical situation, suggesting that higher levels might be needed to optimally support preterm neonates with RDS.