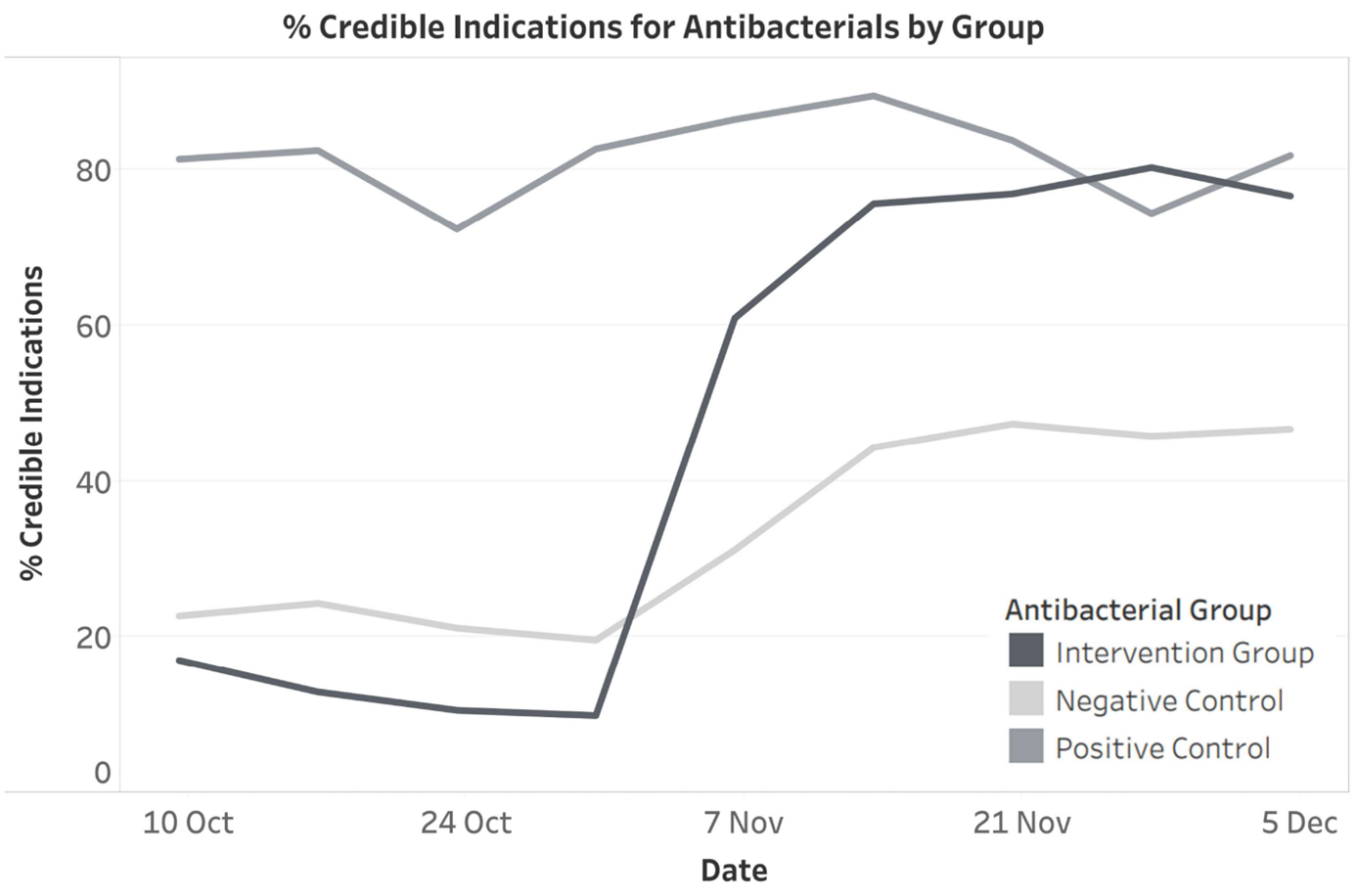
Aim Indications for medicines are poorly recorded in prescriptions at our hospitals. Indications are ‘optional’ on paper prescriptions but can be mandated in electronic prescriptions. As part of an initiative to improve indication documentation for antimicrobial medicines, a prospective controlled study of compulsory indications for antibacterial medicines was undertaken. Our aim was to assess the effect of making indications compulsory in an electronic prescribing and administration (ePA) system. Methods Compulsory indications on prescriptions were implemented in our tertiary hospital ePA system for eight antibacterial medicines. The proportion of ‘credible indications’ following the intervention for these medicines was compared with 23 antibacterial medicines with pre-existing (positive control) and 71 without (negative control) compulsory indications. Documented indications for all antibacterial medicines four weeks before and after implementation of compulsory indications were extracted from the ePA system and manually classified as ‘credible indication’, ‘other text’, ‘rubbish text’, or ‘blank’. Results The proportion of ‘credible indications’ for the intervention group had an absolute increase of 64.8%, from 12.5% (270/2166) to 77.3% (1684/2179). In the intervention group ‘rubbish text’ increased by 1.3% (from 0.05% to 1.3%), ‘other text’ increased from 5.4% to 15.3%, and ‘blank’ decreased from 82.1% to 6.1%. For antibacterials with no compulsory indication ‘credible indications’ increased from 22.0% (793/3611) to 46.0% (1667/3621), and in those with pre-existing compulsory indications from 80.3% (191/238) to 83.2% (183/220). Conclusion Implementation of compulsory indications for antibacterial medicines in the ePA system increased ‘credible indications’ substantially with a small increase in ‘rubbish text’.