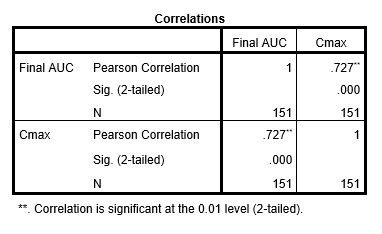
OBJECTIVES: The primary objective of this study was to compare the therapeutic predictive value of area under the curve (AUC24) versus maximum concentration (Cmax) in cystic fibrosis (CF) patients receiving intravenous (IV) tobramycin for a Pseudomonas aeruginosa (PsA) acute pulmonary exacerbation (APE). Acute kidney injury (AKI) incidence and the relationship between time undetectable and efficacy were also assessed. METHODS: A retrospective review was conducted in patients aged at least one month with a diagnosis of CF receiving IV tobramycin for treatment of a PsA APE and admitted to the University of Kentucky between August 2015 and August 2019 . Patients were excluded if they had no growth of PsA on sputum culture or if two post-dose tobramycin levels were not obtained following a dose adjustment of ≥20%. RESULTS: A total of 44 pediatric and 107 adult patient encounters met inclusion criteria. In patients with therapeutic success (n=91), 75.8% had an AUC24 ≥80 and 80.3% had a Cmax ≥8 times the highest PsA minimal inhibitory concentration (MIC). There was a significant correlation between AUC24 and Cmax (r2 = 0.727; p<0.001). AKI incidence was significantly higher in patients receiving IV tobramycin dosed multiple times daily versus at least every 24 hours (50% versus 28.7%; p=0.047). CONCLUSIONS: The results of this study indicate that both AUC24 and Cmax serve as relatively accurate predictors of tobramycin efficacy. Additionally, given the significant increase in incidence of AKI, multi-daily dosing of IV tobramycin should be used only in select pediatric and adult patients with CF.