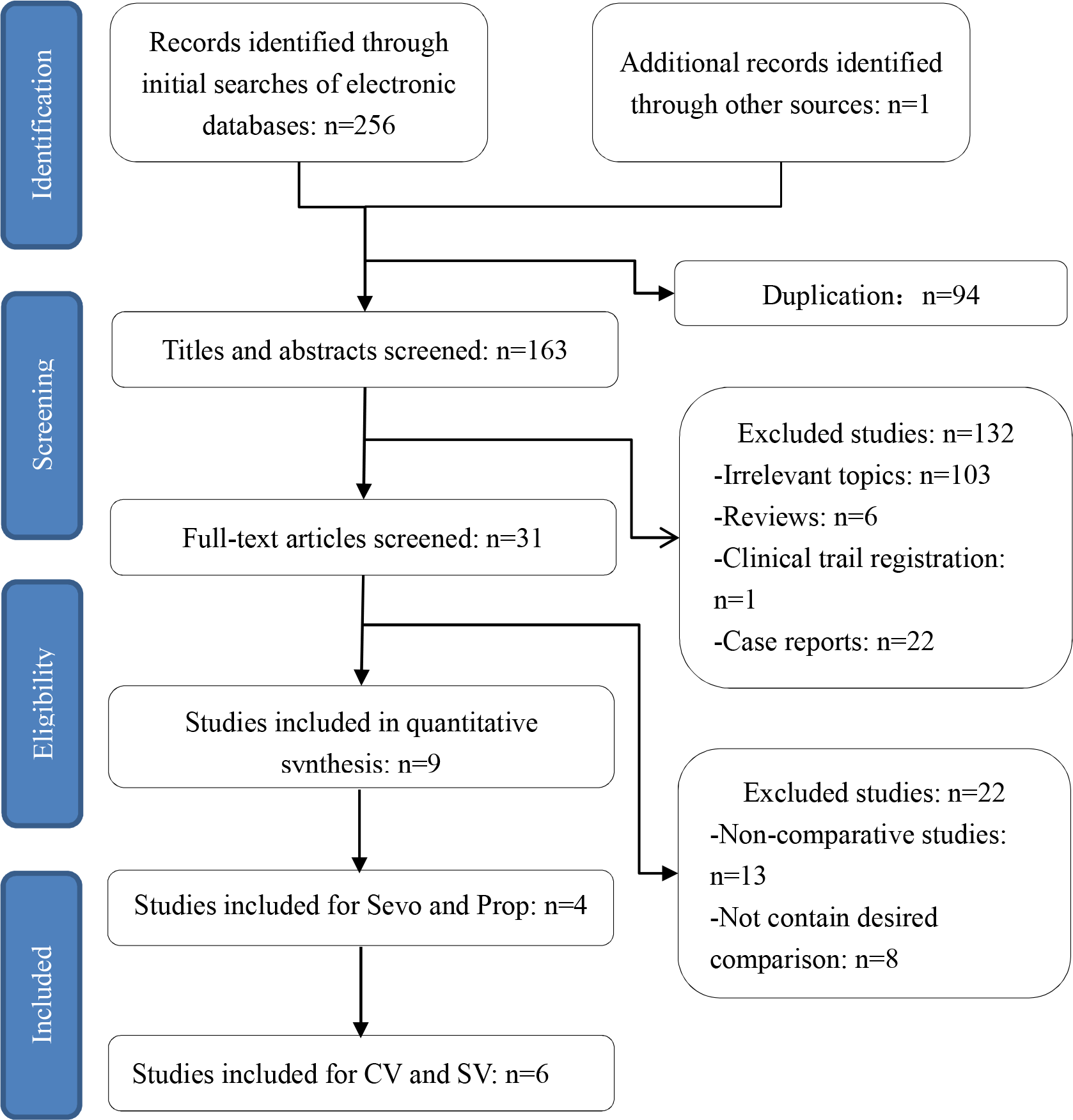
Background: There is no consensus regarding the optimal anesthetic approach to rigid bronchoscopy in children suffering from tracheobronchial FBA. We performed this meta-analysis to assess the efficacy and safety of the different anesthesia agents and ventilation modes for tracheobronchial foreign body removal via rigid bronchoscopy in young children. Methods: A systematic search of three major databases for all relevant articles. A meta-analysis was performed to analyze the data. Results: Four trials for evaluating different anesthetics and six trials for evaluating two kinds of ventilation modes were found. Compared with the sevoflurane-based volatile anesthesia group , the rate of perioperative complications included hypoxemia (OR, 2.07; 95% CI, 1.38–3.11; P=0.0004; I2 = 0%), apnea (OR, 2.74; 95% CI, 1.11–6.78; P = 0.03; I2 = 60%), laryngospasm (OR, 2.89; 95% CI, 1.67–4.98; P=0.0001; I2 = 0%), cough/bucking (OR, 2.93; 95% CI, 1.86–4.63; P<0.00001; I2 = 0%), and body movement (OR, 3.51; 95% CI, 2.03–6.09; P<0.00001; I2 = 0%) were significantly increased in the propofol-based total intravenous anesthesia and the duration of operation were longer in the Group Prop. Compared with the control ventilation group , the incidences of laryngospasm (OR, 0.16; 95% CI, 0.05–0.56; P=0.004; I2 = 54%), apnea (OR, 0.21; 95% CI, 0.09–0.50; P=0.0004; I2 = 0%), and cough/bucking (OR, 0.03; 95% CI, 0.01–0.10; P<0.00001; I2 = 41%) increased in the spontaneous ventilation group and the duration of operationand emergence from anesthesia significantly prolonged in the Group SV. Conclusions: Our meta-analysis suggests that sevoflurane-based volatile anesthesia was superior to propofol-based total intravenous anesthesia for the management of foreign body aspiration in children. There is still no strong evidence indicated that one ventilation technique was superio