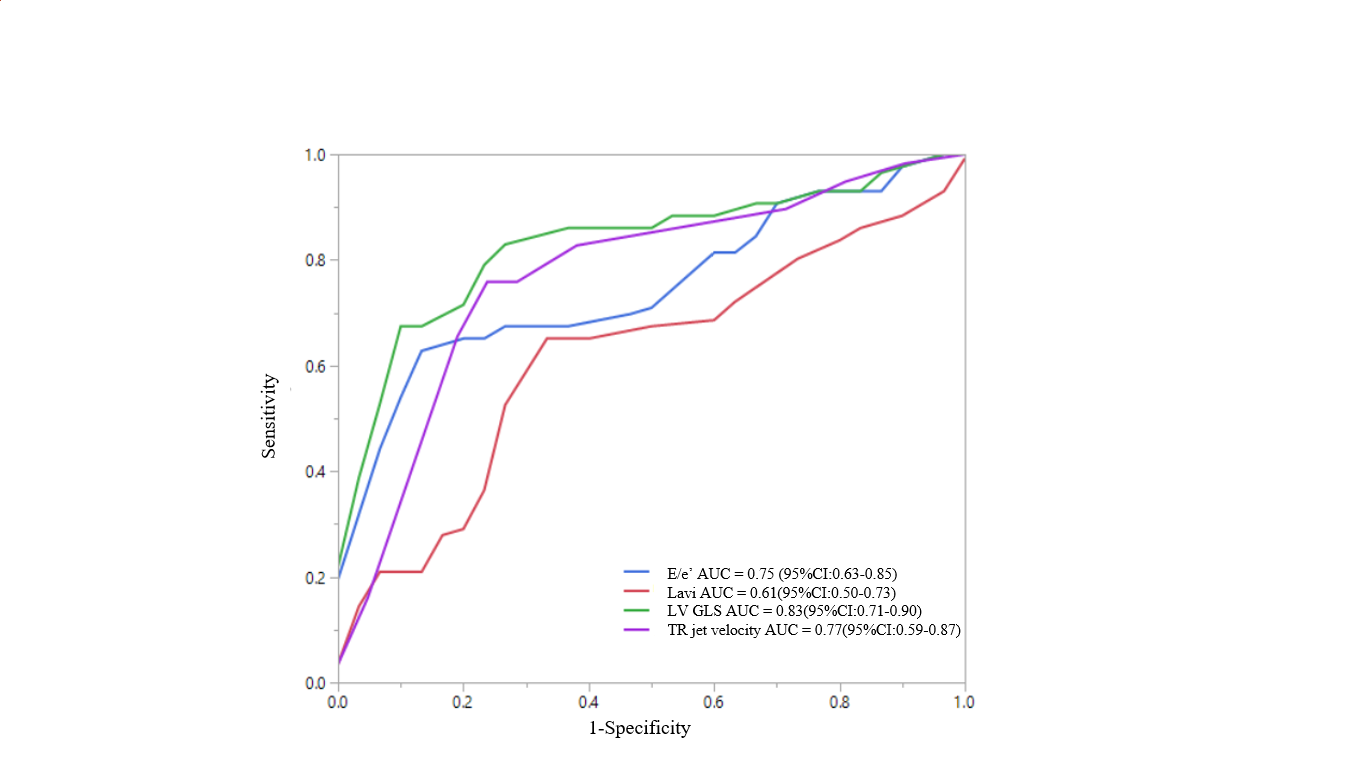
Purpose: An elevated left ventricular (LV) filling pressure is the main finding in patients with heart failure with preserved ejection fraction, which is estimated with an algorithm using echocardiographic parameters recommended by the recent American Society of Echocardiography (ASE)/European Association of Cardiovascular Imaging (EACVI) guideline. In this study, we sought to determine the efficacy of LV global longitudinal strain (GLS) to estimate the elevated LV filling pressure. Methods and Results: 73 prospectively selected patients undergoing left ventricular catheterization (mean age 63.19±9.64, 68.5% male) participated in this study. Using the algorithm, the LV filling pressure was estimated with the echo parameters obtained within 24hrs before the catheterization. The LV GLS was measured using the automated functional imaging system (GE, Vivid E9 USA). Invasive LV pre-A pressure corresponding to mean left atrial pressure (LAP) was used as a reference, and >12 mm Hg was defined as elevated. The invasive LV filling pressure was elevated in 43 (58.9%) and normal in 30 patients (41.1%). In 9 (12.3%) patients of 73 are defined as indeterminate based on the 2016 algorithm. Using the ROC method, -18.1% of LV GLS estimated the LV filling pressure (AUC=0.79, 73% specificity, 84% sensitivity) with higher sensitivity compared with the algorithm (AUC=0.76, 77% specificity, 72% sensitivity). Conclusions: We confirmed that the LV GLS is feasible and reproducible in estimating LV filling pressure. In addition, LV GLS highly predicts elevated LAP as E/e’ and TR jet velocity and may be used as major criteria for the diagnosis of HFpEF