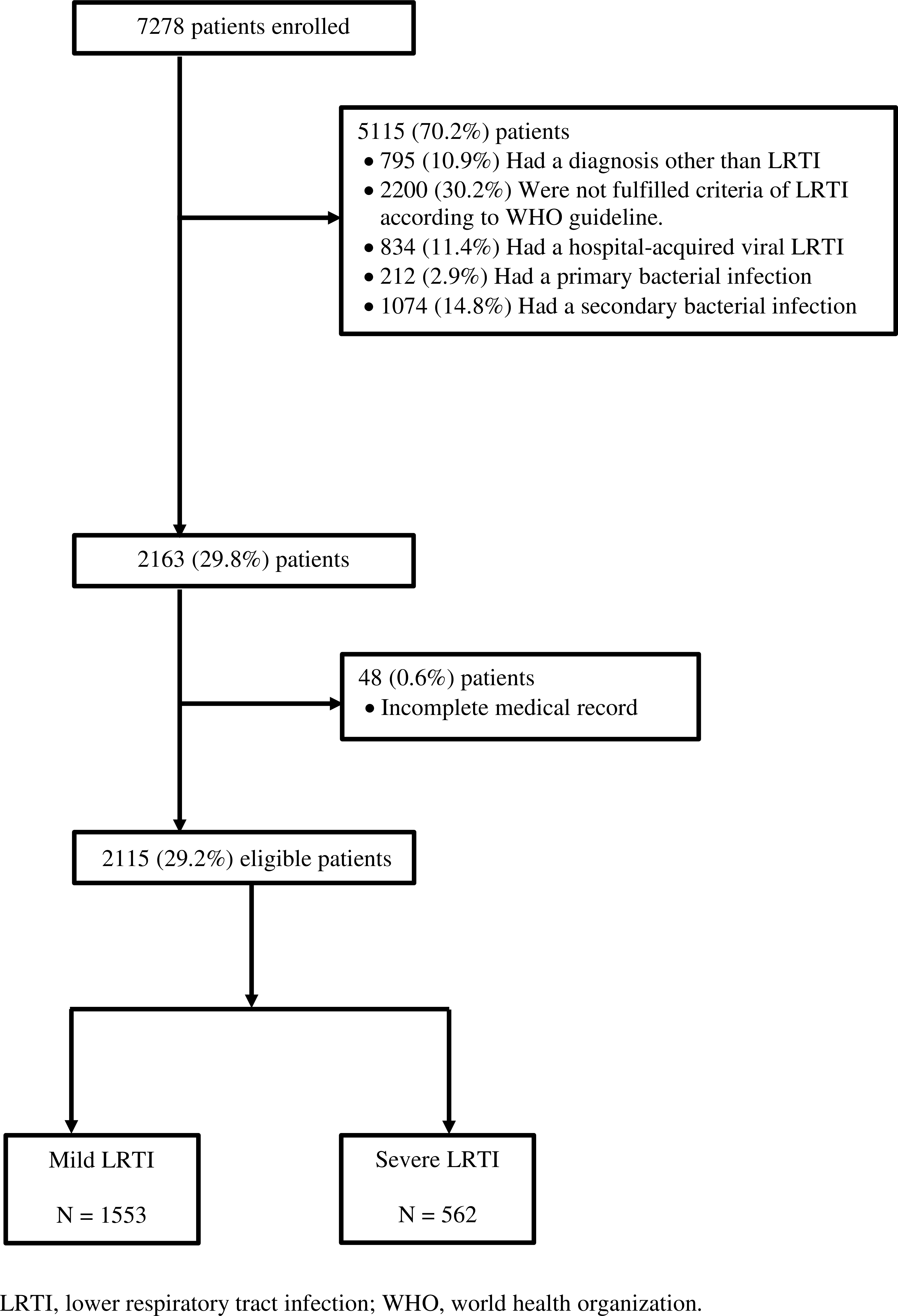
Objective: To determine whether viral coinfection is a risk for severe lower respiratory tract infection (LRTI). Working Hypothesis: Children with viral coinfection had a higher risk for admission to the intensive care unit (ICU) than those with a single virus infection. Study Design: Retrospective, observational study for ten years. Patient-Subject Selection: Children between 1-60 months of age hospitalized with LRTI. Methodology: We defined severe LRTI as admission to the ICU for high-flow nasal cannula oxygen/bilevel positive airway pressure/invasive ventilation and assessed demographic and laboratory data with potential risk factors from the patients’ medical records. Results: Of 2115 children hospitalized with LRTI, 562 had severe, and 1553 had mild disease. Viral coinfection was present in 28.3% of all patients, and those with viral coinfection were at a higher risk of severe LRTI than those with a single virus infection (43.8% vs. 22.7%; aOR, 3.44; 95% CI, 2.74-4.53). Respiratory syncytial virus (RSV) and rhinovirus (except for between 25-60 months) coinfections were associated with severe LRTI in all ages, whereas parainfluenza virus-3 (PIV3; 7-24 months) and bocavirus (7-12 months) coinfections led to severe LRTI in early childhood. Moreover, influenza-A coinfection caused severe LRTI in children between 7-12 and 25-60 months. Other risk factors included young age, prematurity, history of atopy, exposure to tobacco smoke, underlying condition, neutrophilia, lymphopenia, and high CRP value. Conclusion: Children with viral coinfection, particularly with rhinovirus, RSV, influenza-A, PIV3, and bocavirus, may be followed closely regarding the clinical changes.