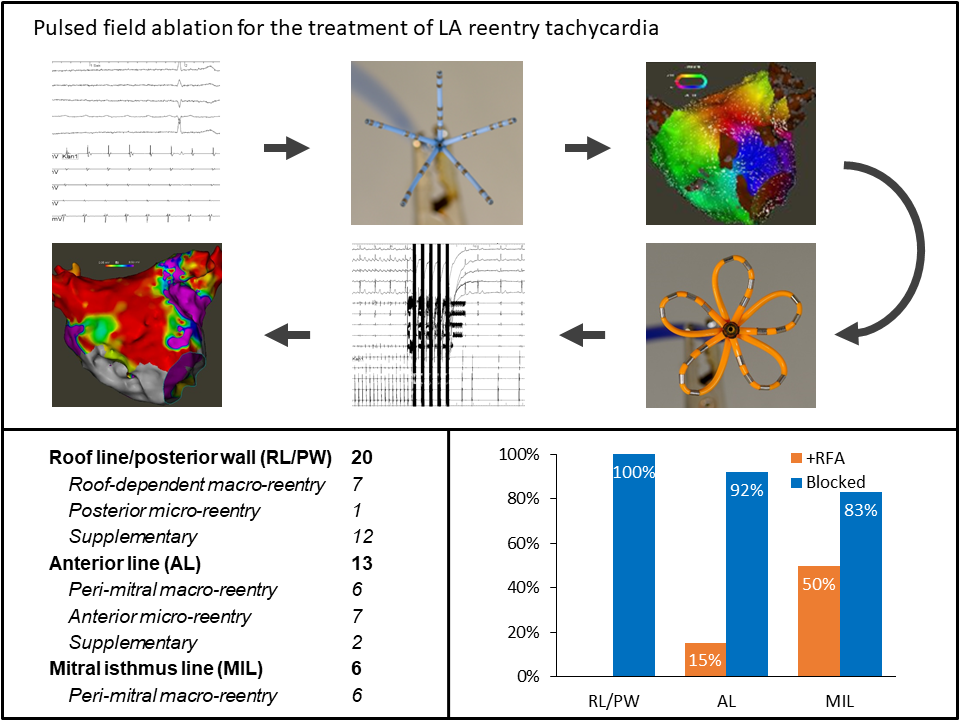
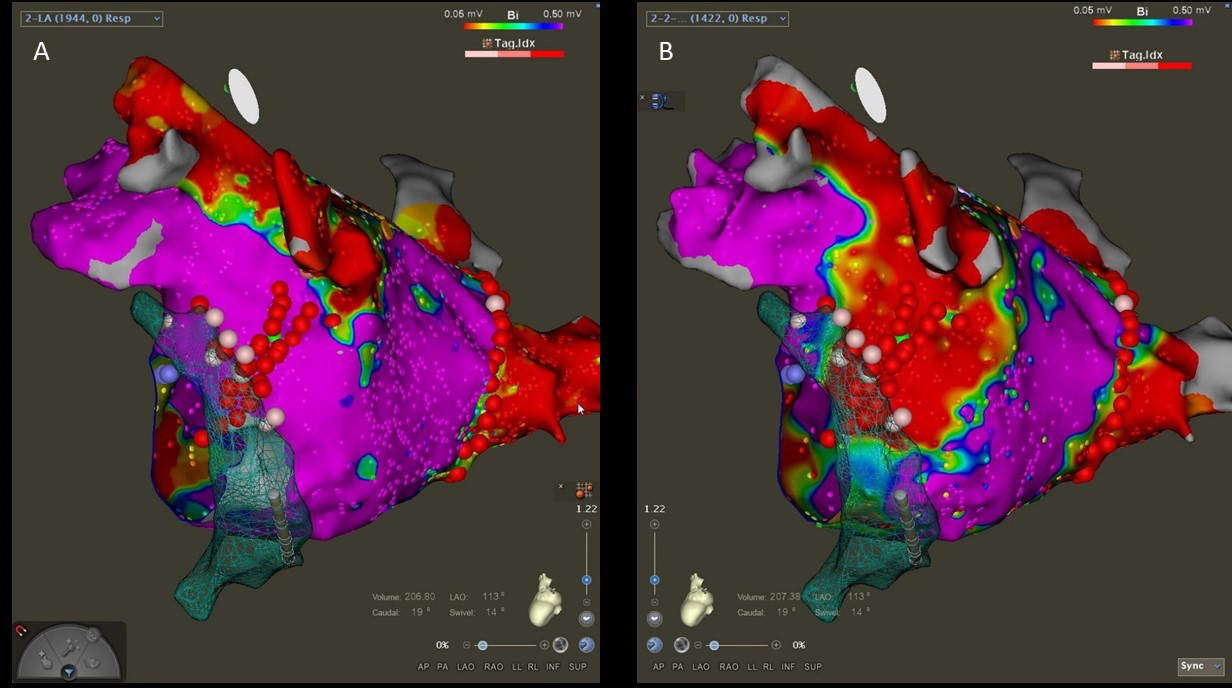
Aims A multipolar pulsed-field ablation (PFA) catheter was recently introduced for pulmonary vein isolation and shows great promise with respect to procedural efficacy and safety. We describe our initial experience using this multipolar PFA catheter for the treatment of left atrial (LA) reentry tachycardia. Methods We included all patients with LA reentry tachycardia treated with PFA at our institution between September 2021 and March 2022. The tachycardia mechanism was identified using 3D electro-anatomical mapping (3D-EAM). Subsequently, a roof line, anterior line, or mitral isthmus line was ablated as appropriate. Roof line ablation was always combined with LA posterior wall (LAPW) isolation. Supplementary ablation of a roof- or anterior line was added in patients with extensive low-voltage areas to avoid future arrhythmias. Positioning of the PFA catheter was guided by a 3D-EAM system, and by fluoroscopy. Bidirectional block across lines was verified using standard criteria. Additional focal radiofrequency ablation (RFA) was used to achieve bidirectional block as necessary. Results Among 22 patients (median age 70 (59-75) years; 9 females), we identified 27 LA reentry tachycardia: Seven roof dependent macro-reentries, one micro-reentry located on the posterior wall, twelve peri-mitral macro-reentries, and seven micro-reentries located on the anterior wall. We ablated a total of 20 roof lines, 13 anterior lines and 6 mitral isthmus lines. Additional RFA was necessary for two anterior lines (15%) and three mitral isthmus lines (50%). Bidirectional block was achieved across all roof lines, 92% of anterior lines and 83% of mitral isthmus lines. We observed no acute procedural complications. Conclusion Ablation of a roof line and LAPW isolation is feasible, effective and safe using this multipolar PFA catheter. However, the catheter is less suited for ablation of the mitral isthmus and the anterior line. A focal pulsed-field ablation catheter may be more effective for ablation of these lines.