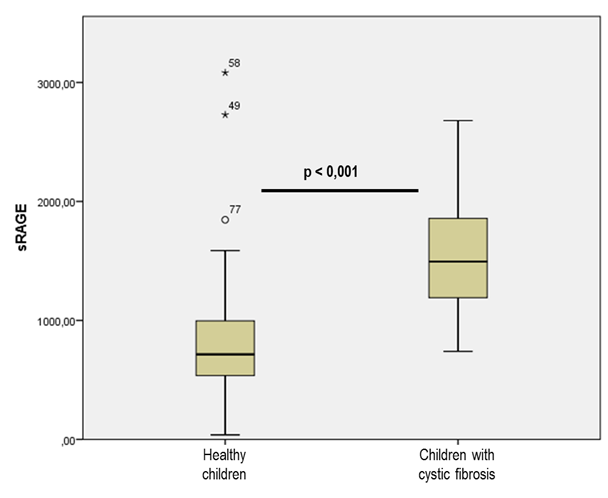
The receptor for advanced glycation end products (RAGE) has been studied in several respiratory diseases described as an important inflammatory mediator. The RAGE-axis is activated by multiple endogenous ligands related to pro-inflammatory states, upregulate the RAGE expression. The function of soluble RAGE (sRAGE) is not completely understood, it has been hypothesized an anti-inflamatory role as RAGE decoy receptor. Few studies have explored the RAGE-axis in Cystic Fibrosis (CF) with contradictory results. Based on previously, we present this pilot study with the aim of describe the plasma sRAGE levels in children with cystic CF (CFp), compare with the sRAGE levels in a healthy cohort and study its possible correlation with CFp clinical features. We conducted a single-center, cross-sectional observational study. We included 35 clinically stable CF patients (aged < 18 years). The median plasma sRAGE level in CFp was 1494,75 pg/ml [interquartile range (IQR) 708,75pg/ml], compared with 714,20 pg/ml (IQR 490,50 pg/ml)) in the historical cohort of healthy controls (p < 0,001). A positive correlation was found between plasma sRAGE level and forced expiratory volume in 1 second/forced vital capacity ratio (FEV1/FVC) (p 0,004) and forced expiratory flow between 25% and 75% (FEF25%-75%) (p 0,032). In this preliminary study, the plasma sRAGE level were higher in CFp than in healthy controls. Also, we described a positive correlation between FEV1/FVC and FEF25%-75% and plasma sRAGE. To our knowledge, our study is the largest to describe plasma sRAGE values in CFp and the only one carried out in pediatric CF population.