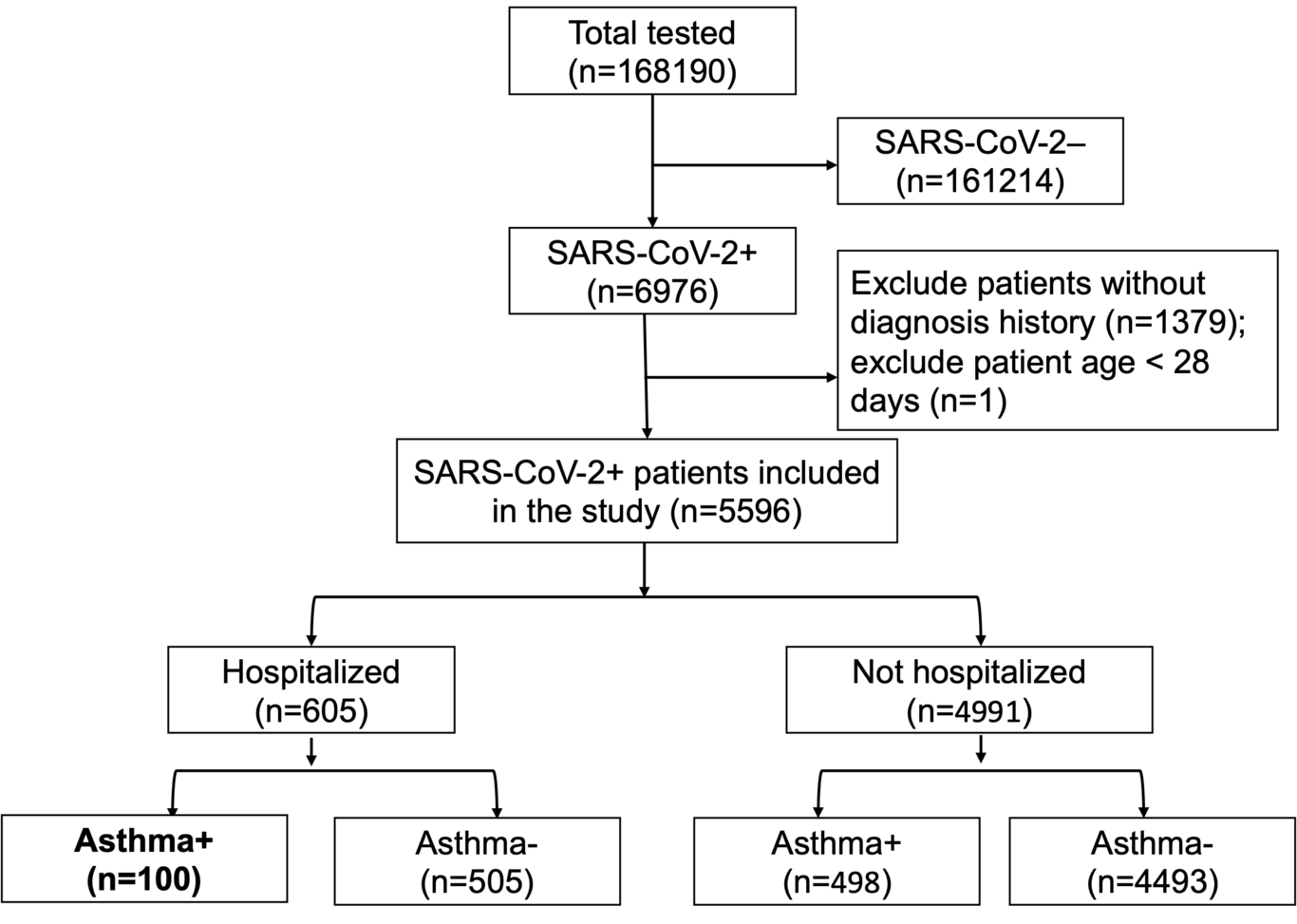
Background: It is unclear if asthma and its allergic phenotype are risk factors for hospitalization or severe disease from SARS-CoV-2. Methods: All patients testing positive for SARS-CoV-2 between March 1 and September 30, 2020, were retrospectively identified and characterized through electronic analysis at Stanford. A sub-cohort was followed prospectively to evaluate long-term COVID-19 symptoms. Results: 168,190 patients underwent SARS-CoV-2 testing, and 6,976 (4·15%) tested positive. In a multivariate analysis, asthma was not an independent risk factor for hospitalization (OR 1·12 [95% CI 0·86, 1·45], p=0·40). Among SARS-CoV-2 positive asthmatics, allergic asthma lowered the risk of hospitalization and had a protective effect compared to non-allergic asthma (OR 0·52 (0·28, 0·91), p=0·026); there was no association between baseline medication use as characterized by GINA and hospitalization risk. Patients with severe COVID-19 disease had lower eosinophil levels during hospitalization compared to patients with mild or asymptomatic disease, independent of asthma status (p=0.0014). In a patient sub-cohort followed longitudinally, asthmatics and non-asthmatics had similar time to resolution of COVID-19 symptoms, particularly lower respiratory symptoms. Conclusions: Asthma is not a risk factor for more severe COVID-19 disease. Allergic asthmatics were half as likely to be hospitalized with COVID-19 compared to non-allergic asthmatics. Lower levels of eosinophil counts (allergic biomarkers) were associated with more severe COVID-19 disease trajectory. Recovery was similar among asthmatics and non-asthmatics with over 50% of patients reporting ongoing lower respiratory symptoms three months post-infection.