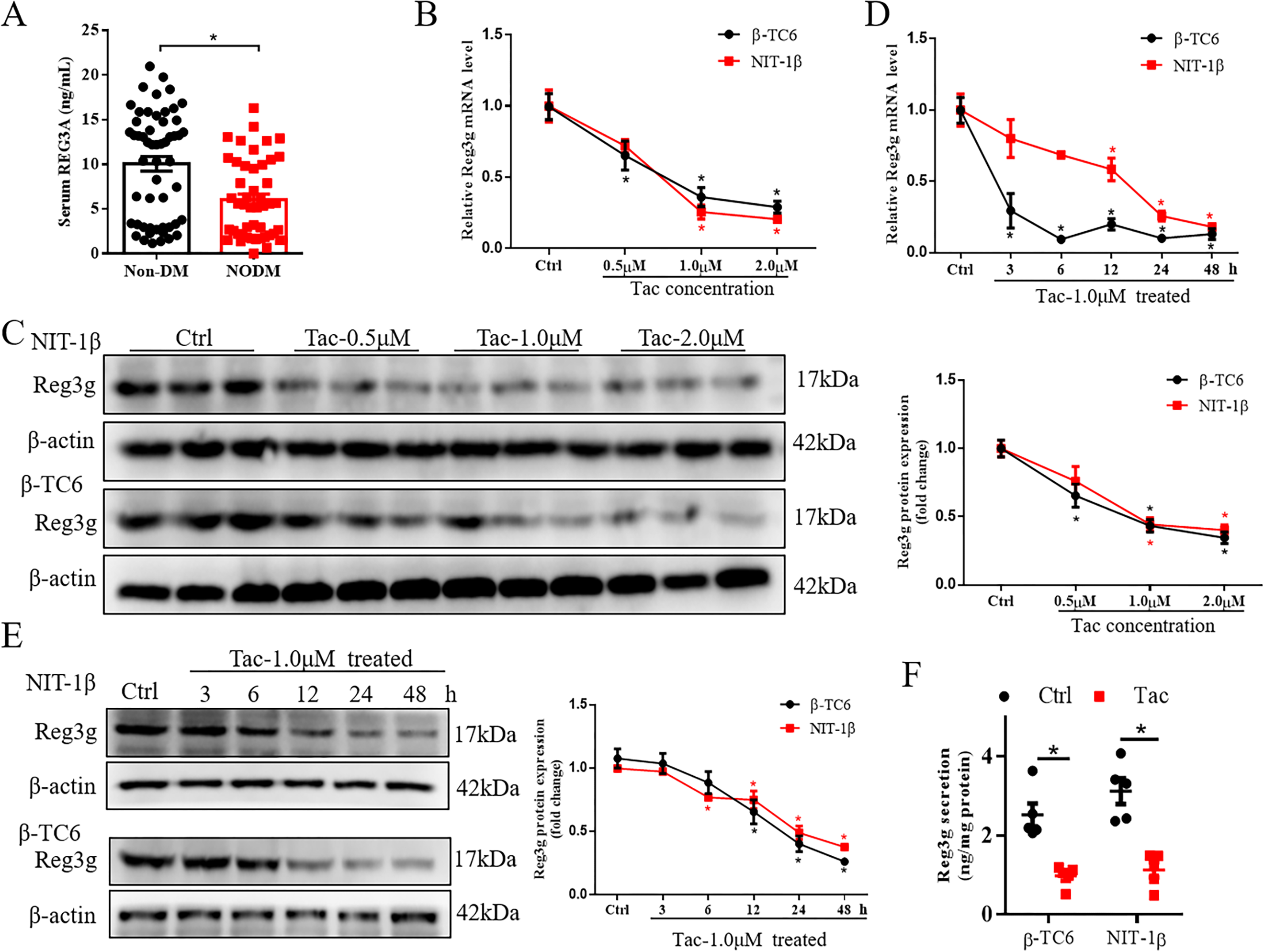
Background and Purpose: Tacrolimus (Tac) induces pancreatic β cell dysfunction, causing new-onset diabetes mellitus (NODM) after transplantation. Reg3g is a member of the pancreatic regenerative gene family, as reported to improve type 1 diabetes by promoting β cell regeneration. Here, we aim to investigate the role and approach of Reg3g in reversing Tac-induced β cell dysfunction and NODM in mice. Experimental Approach: Circulating REG3A (the human homolog of mouse Reg3g) concentrations of patients treated with Tac after heart transplantation(HT) were detected. The glucose-stimulated insulin secretion (GSIS) and mitochondrial functions, including mitochondria membrane potential (MMP), mitochondria calcium uptake, ATP production, and oxygen consumption rate (OCR), were tested in β cells. Effects of Reg3g on Tac-induced NODM in mice were studied. Key Results: Circulating REG3A levels significantly decreased in NODM patients treated with Tac compared with those without diabetes. Tac down-regulated Reg3g via inhibiting STAT3-mediated transcription activation, while Reg3g protected against Tac-induced apoptosis of β cells. Besides, Reg3g restored GSIS suppressed by Tac in β cells via improving mitochondrial function, including increased MMP, mitochondria calcium uptake, ATP production, and OCR. Mechanically, Reg3g increased accumulation of pSTAT3(Ser727) in mitochondria by activating ERK1/2-STAT3 signaling pathway, leading to restoration of Tac-caused mitochondrial impairment. Moreover, Reg3g overexpression effectively ameliorated Tac-induced NODM in mice. Conclusion and Implications: Reg3g ameliorates Tac-induced pancreatic β cell dysfunction by restoring mitochondrial function via a pSTAT3(Ser727)-dependent way. Our observations identify a novel Reg3g-involved mechanism underlying the augmented incidence of Tac-induced NODM and reveal that Reg3g ameliorates Tac-induced β cell dysfunction.