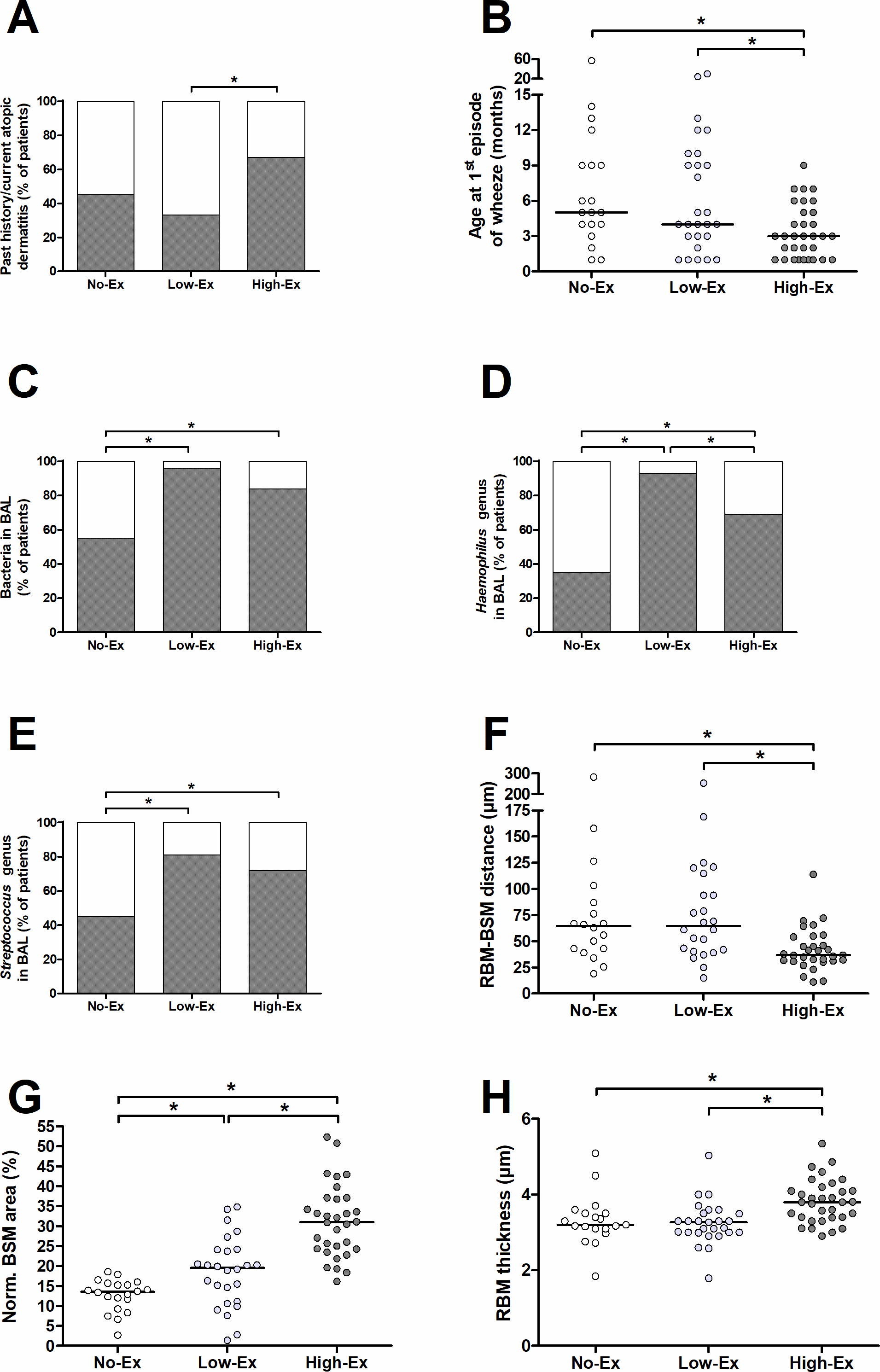
INTRODUCTION: Exacerbations in preschool wheezers increase the risk of impaired lung function and asthma persistence at school age. Bronchial remodelling-based latent classes identify severe preschool wheezers at increased risk of frequent exacerbations (>3) but failed to distinguish those without exacerbation from those with low exacerbations rate (1-2 exacerbations) in the year following bronchoscopy. We thus aimed to identify further independent factors associated with no, low or high exacerbation rates. METHODS: In this post-hoc analysis, 80 severe preschool wheezers from the “P’tit Asthme” and “RESPIRE” studies were divided into 3 groups: No-Ex (0 exacerbation in the year following the bronchoscopy, n=20), Low-Ex (1-2 exacerbations, n=27) and High-Ex (≥3 exacerbations, n=33). Associations between variables and groups were assessed using multinomial logistic regressions. RESULTS: Atopic dermatitis, age at the first wheezing episode, Haemophilus and Streptococcus genera in the bronchoalveolar lavage fluid (BALF), bronchial smooth muscle (BSM) area, reticular basement membrane (RBM) thickness and RBM-BSM distance were all significantly different between No-Ex and/or Low-Ex and/or High-Ex. However, only atopic dermatitis, age at first episode of wheezing, Haemophilus genus in the BALF, RBM-BSM distance and BSM area were significantly and independently associated with exacerbation frequency. Among them, the BSM area was the sole parameter independently associated with each group. CONCLUSION: While atopic dermatitis, age at the first episode of wheezing, Haemophilus in BALF, RBM-BSM distance and BSM area appeared to be relevant independent parameters associated with exacerbation susceptibility in severe preschool wheezers, only the increased BSM area discriminated between each of the three-exacerbation frequency-based groups.