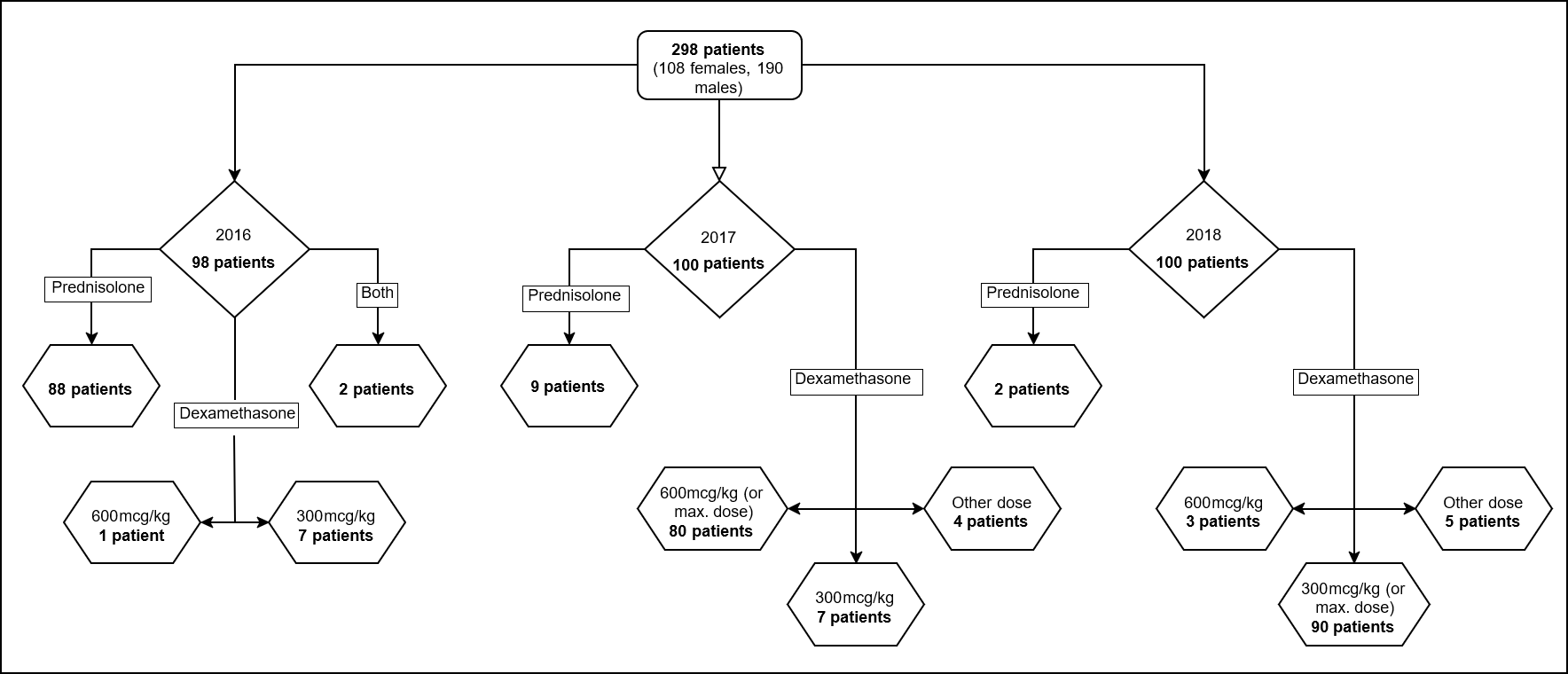
Background & local problem: Acute wheezing attacks are a leading cause of Pediatric Emergency Department (PED) attendances and inpatient admissions and are a considerable burden on the healthcare providers. Almost one-third of children vomit prednisolone in the PED, requiring anti-emetics and repeat dosing. Aim: This quality improvement (QI) intervention aimed to improve oral corticosteroid (OCS) tolerability, reduce emergency department length of stay (LOS), and reduce OCS drug costs for acute wheeze attendances in a PED, while not adversely affecting admissions, re-attendance, or mortality rates. QI Interventions: Included (1) a departmental protocol and (2) modification of the OCS type and dosage from prednisolone (3-day course of 1 mg/kg) to dexamethasone (600 mcg/kg, then single dose 300 mcg/kg). Methods: The study team reviewed the evidence and implemented the interventions. To assess the scale of improvement, we retrospectively collected data on attendance records for patients aged 2-14 years with acute wheeze requiring OCS. We collected data on 100 children who attended the PED between October and December for each year (2016, 2017, and 2018). We then assessed OCS tolerability, LOS, OCS drug costs, and, admission, re-attendance, and mortality rates. Results: Over a 48-month period, we increased OCS tolerability by 67.2% and achieved an 85.8% reduction in OCS drug costs (saving £41,553.14). There was no change in the LOS, admission, re-attendance, and mortality rates. Conclusions: Improved tolerability and substantial cost savings can be achieved by implementing a structured acute pediatric wheeze protocol and modifying the OCS to single-dose dexamethasone (300 mcg/kg).