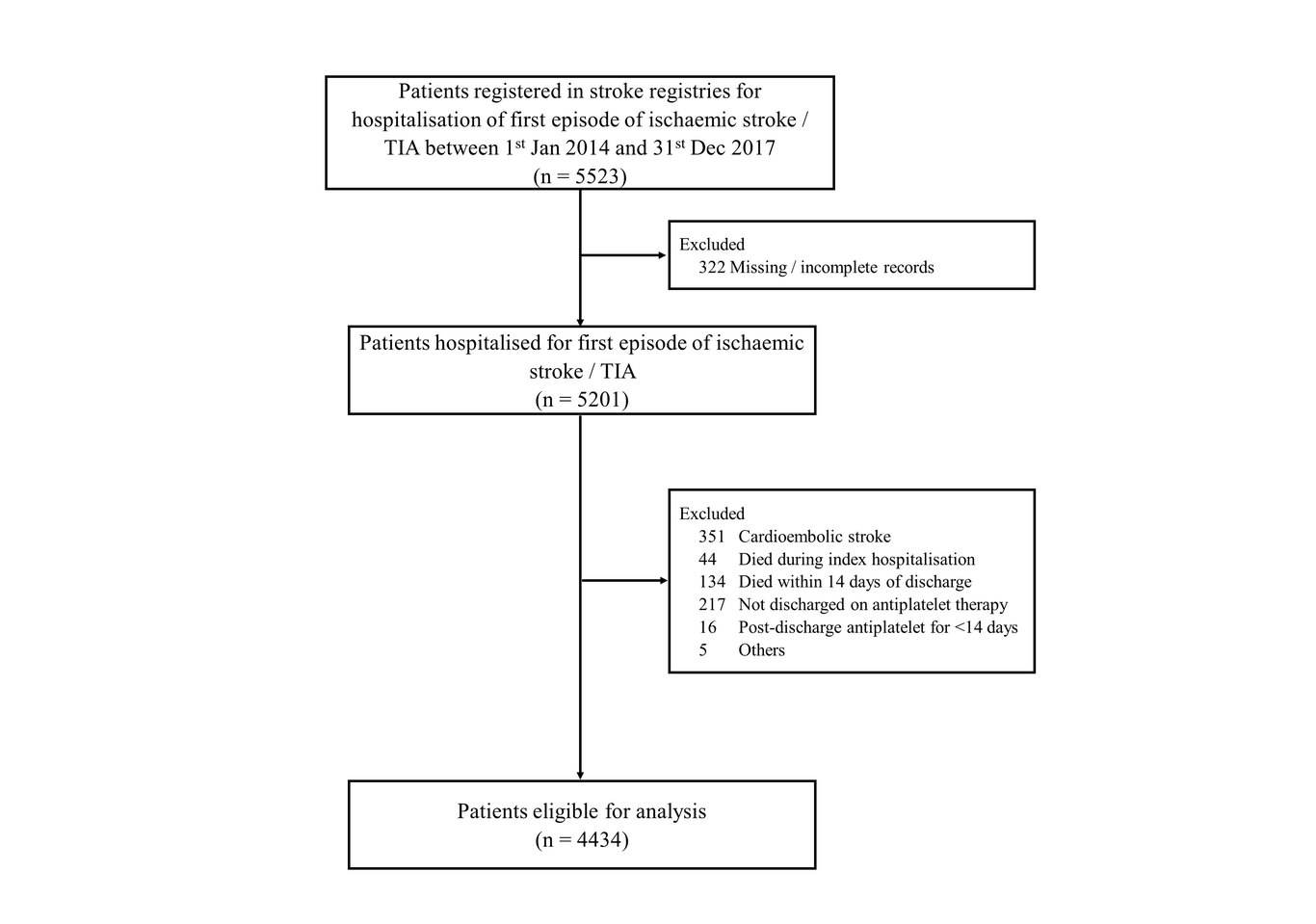
Objective: This study aimed to assess effectiveness and safety outcomes of antiplatelet therapy for secondary prevention among patients with ischaemic stroke or transient ischaemic attack (TIA) in Malaysia. Method: Patients with a first ischaemic stroke/TIA between 2014 and 2017 were identified from stroke registry and data was linked with other data sources for information on antiplatelet exposure and outcome events. Exposure was defined as antiplatelet therapy at discharge from the index stroke hospitalisation and categorised into single antiplatelet therapy (SAPT) and dual antiplatelet therapy (DAPT) groups. Primary outcome was composite events of stroke, myocardial infarction, and all-cause death at up to one year after the index stroke in an intention-to-treat analysis. Results: Of 4434 patients included in the analysis, 6.7% were treated with DAPT and 93.3% were in SAPT group. During the 1-year follow-up, composite events occurred in 5.7% of patients in DAPT group and in 12.3% of SAPT (p<0.001). The rates of individual events were lower in DAPT group compared to SAPT: recurrent stroke (3.4% versus 4.8%), myocardial infarction (0.7% versus 1.9%), and all-cause death (1.7% versus 6.0%). Bleeding occurred in 1.3% of the DAPT group versus 1.6% of the SAPT. Multivariable-adjusted Cox regression analysis showed that rates of composite outcome was lower in the DAPT group compared to SAPT (HR 0.53, 95%CI 0.32, 0.86). Conclusion: In patients with ischaemic stroke/TIA, treatment with DAPT following the index stroke was associated with reduced risk of the composite events of stroke, myocardial infarction, and death. There appears to be similar risk of bleeding with DAPT versus SAPT.