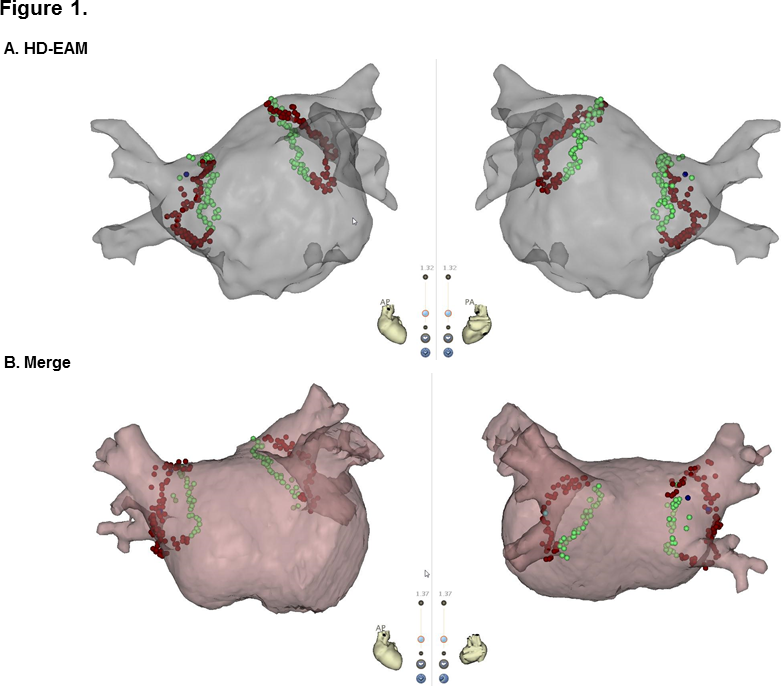
Introduction: Integration of electroanatomical map (EAM) with preacquired three-dimensional (3D) cardiac images provides detailed appreciation of the complex anatomy of the left atrium (LA) and pulmonary vein (PV). High-density (HD) multi-electrode mapping catheters have enabled creating more accurate EAM reflecting real-time volume-rendered LA-PV geometry during atrial fibrillation (AF) ablation. However, no study has compared the outcomes of AF ablation using HD-EAM versus 3D-merged map. We aimed to investigate the procedural and clinical outcomes of AF ablation with HD-EAM (HD-EAM group) versus 3D-merged map (Merge group). Methods: One hundred patients (59.5±11.5years, 53% with paroxysmal AF [PAF]) were randomly assigned (1:1) to HD-EAM or Merged group. HD multi-electrode mapping and contact force (CF)-sensing catheters were used to create virtual LA-PV chamber and to perform wide antral circumferential ablation (WACA), respectively. Results: The two groups showed no significant differences in baseline characteristics and procedural data including ablation time, fluoroscopy time, LA voltage, and CF. PV isolation with a single WACA line was achieved in 21 (42%) and 27 (54%) patients in the Merge and HD-EAM groups, respectively (P=NS). CF was significantly lower in lesions with gap than lesions without gap after a single WACA (7.3±7.3 g vs. 16.0±8.3, respectively, P<0.001). During the 12-month follow-up, no significant difference in AF recurrence was observed between two groups, irrespective of AF type. In multivariate analysis, non-PAF was an independent risk factor for AF recurrence. Conclusion: Integration of 3D cardiac imaging did not improve procedural and clinical outcomes. HD-EAM provides an accurate real-time LA geometry.