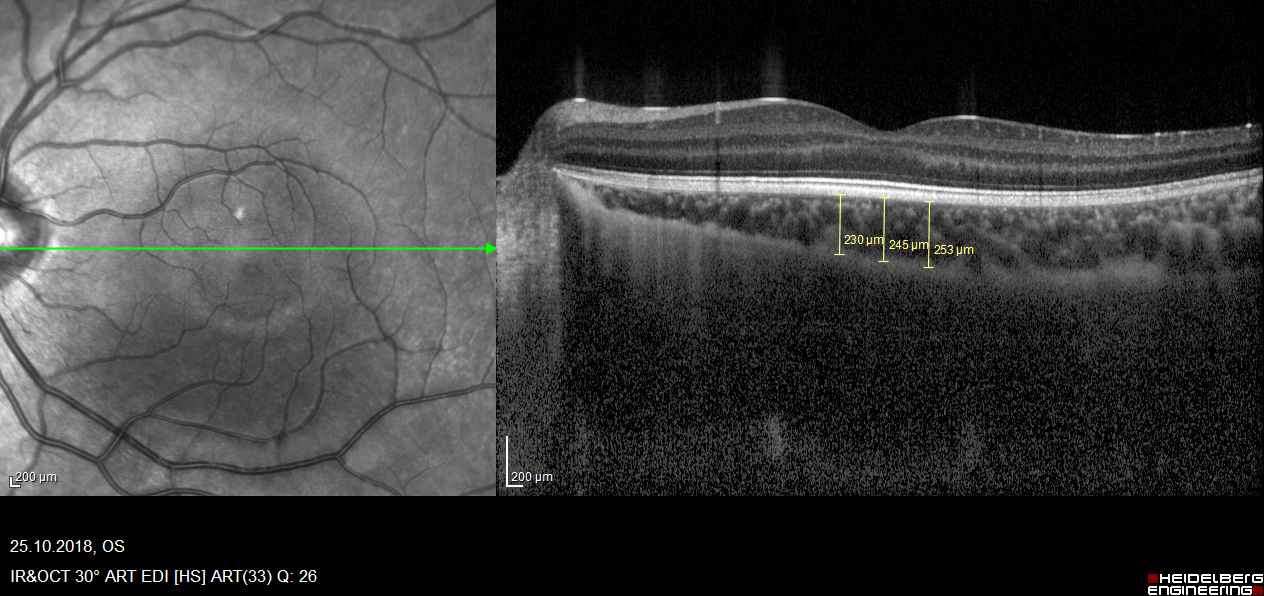
Background: The nonclassic presentation of pediatric celiac disease (CD) becomes increasingly common in daily practice, which requires an awareness of its extraintestinal clinical findings. To evaluate eye involvement and effect of gluten free diet on ocular involvement in pediatric CD patients by measuring the thicknesses of choroid and ganglion cell complex(GCC) composed of retinal nerve fiber layer (RNFL), ganglion cell layer (GCL) and inner plexiform layer (IPL) using enhanced depth imaging optical coherence tomography (EDI-OCT). Methods: Forty-three CD patients aged between four and 16 years (mean age;9.9 ± 4.1, 12 boys and 31 girls), and 48 healthy children (mean age; 11.3 ± 4.1,17 boys and 31 girls) were compared. Following comprehensive eye examinations, thicknesses of choroid at three points and GCC layers (RNFL at five points, GCL and IPL) were obtained using EDI-OCT. Measurement of thicknesses of choroid and GCC layers by a trained EDI-OCT technician and an ophthalmologist who were not aware about group of children in pediatric CD patients with one year gluten free diet. Results: All layers of subfoveal, nasal, temporal choroid were significantly thinner in CD than in the control group (p < .001, p < .001, and p < .001, respectively). No significant difference were observed between the CD and control groups in terms of GCC thicknesses (p > .05). Conclusion: Pediatric CD causing thinning of subfoveal, nasal and temporal areas of choroid, and this change is apparent even after one year gluten free diet. This extraintestinal involvement should be more closely screened at diagnosis and long term clinical results of thin choroid should be determined. Thicknesses of GCC layers were not different in CD group may be revealing the effect of diet or not involvement.