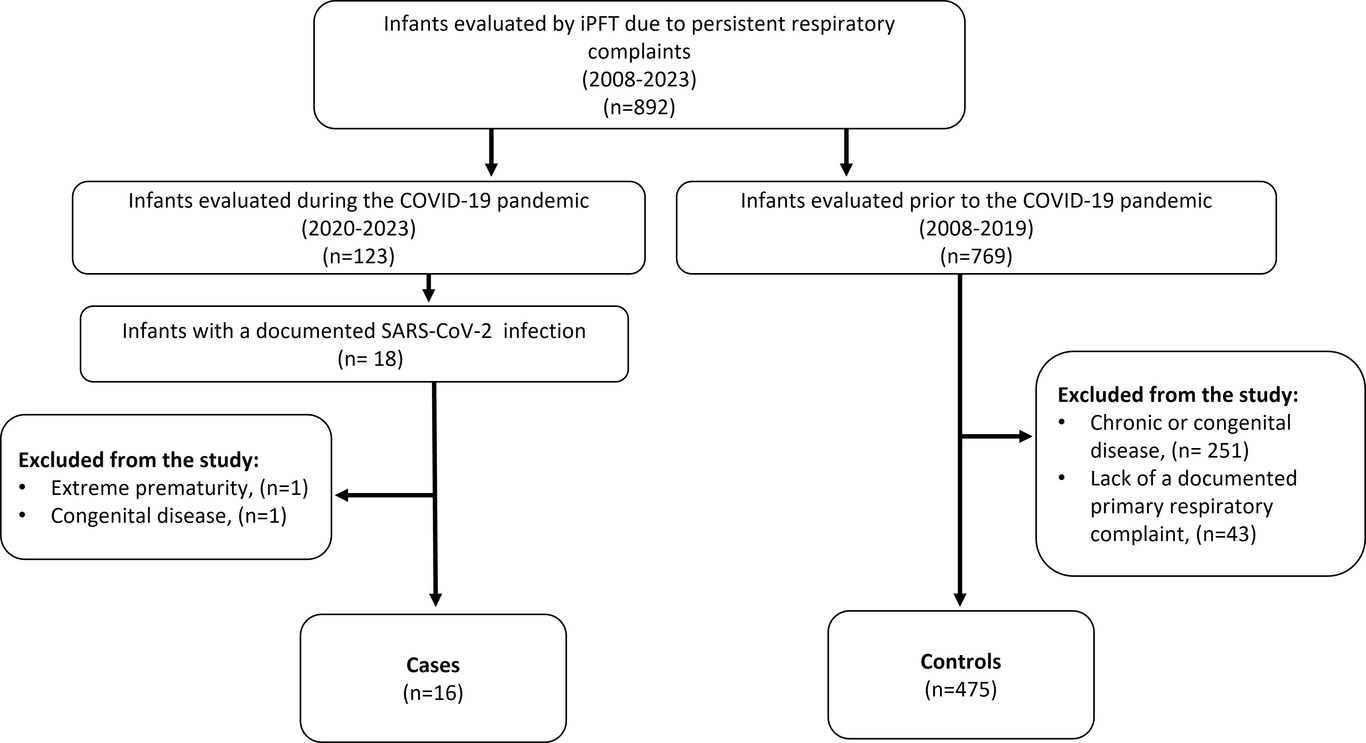
Introduction: The clinical spectrum of SARS-CoV-2 infection is well-established. However, understanding its long-term implications, especially in infants, remains limited. We aimed to evaluate pulmonary function tests in infants (iPFT) several months after a documented SARS-CoV-2 infection. Methods: An observational case-control study was performed. iPFT results in infants with persistent respiratory complaints several months after a SARS-CoV-2 infection were compared to a registry of patients assessed at our center between 2008 and 2019 using the Mann–Whitney U and Fisher’s exact tests. Excluded from the study were infants with chronic diseases and extreme prematurity. Results: iPFT data from sixteen infants with respiratory complaints and a history of SARS-CoV-2 infection and 475 controls were evaluated in the study. The median time between the SARS-CoV-2 infection and iPFT evaluation was 5.5 months (IQR=2.8-8.0). There were no differences between cases and controls in clinical characteristics and reason for iPFT evaluation. iPFT results showed no significant differences between cases and controls in lung volumes, compliance, or resistance. Expiratory airflow limitation was observed in both groups, with better low lung volume flows in the SARS-CoV-2 group. Categorization according to iPFT physiologic alteration and bronchodilator responsiveness were similar in the two groups. Conclusion: This study provides the first comprehensive iPFT data in infants following a SARS-CoV-2 infection. The findings suggest that SARS-CoV-2 infection does not cause unique long-term effects on pulmonary function in infants with chronic respiratory symptoms. Further studies in larger cohorts, particularly in infants with severe acute SARS-CoV-2 infection, are warranted to validate these findings.