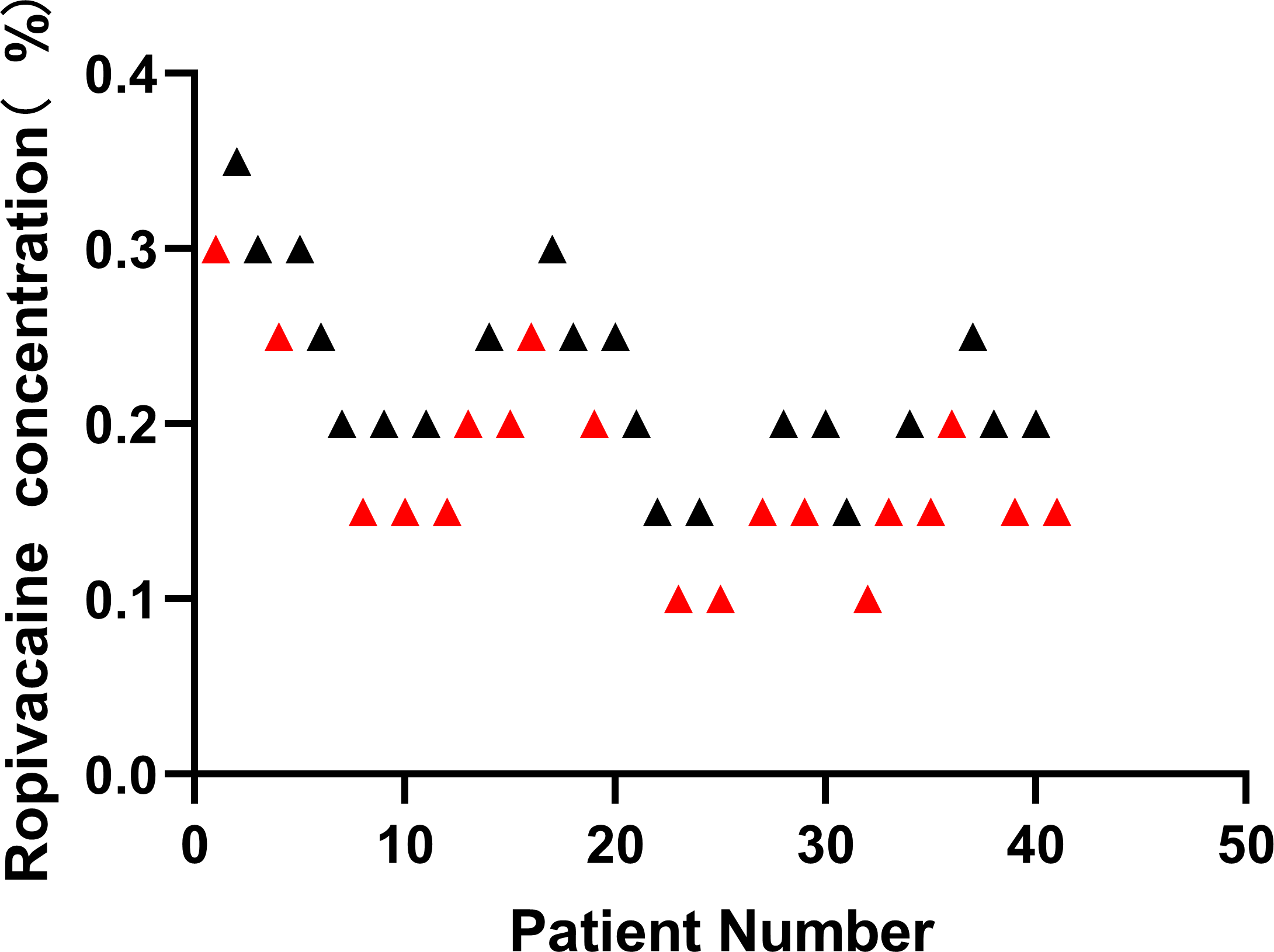
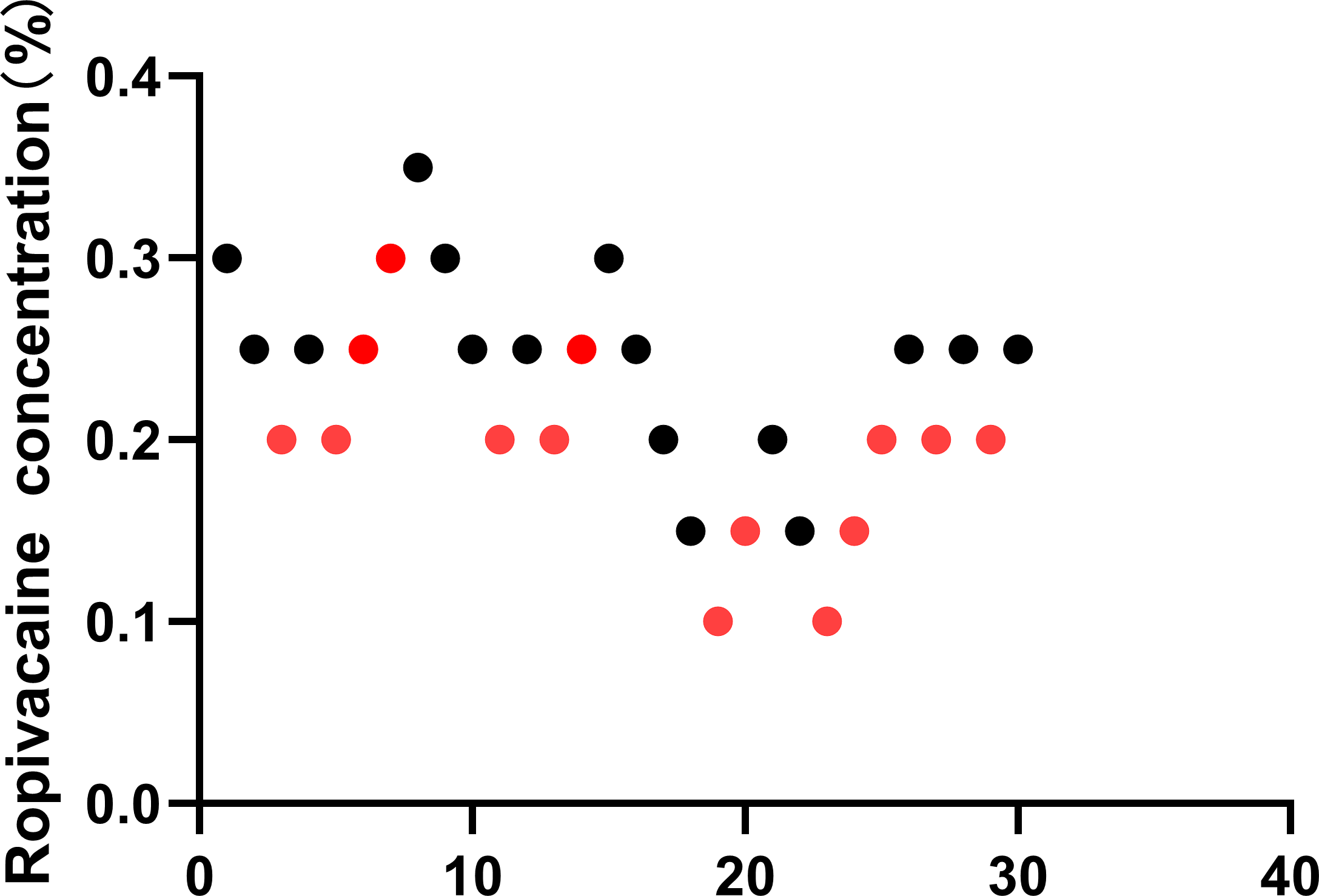
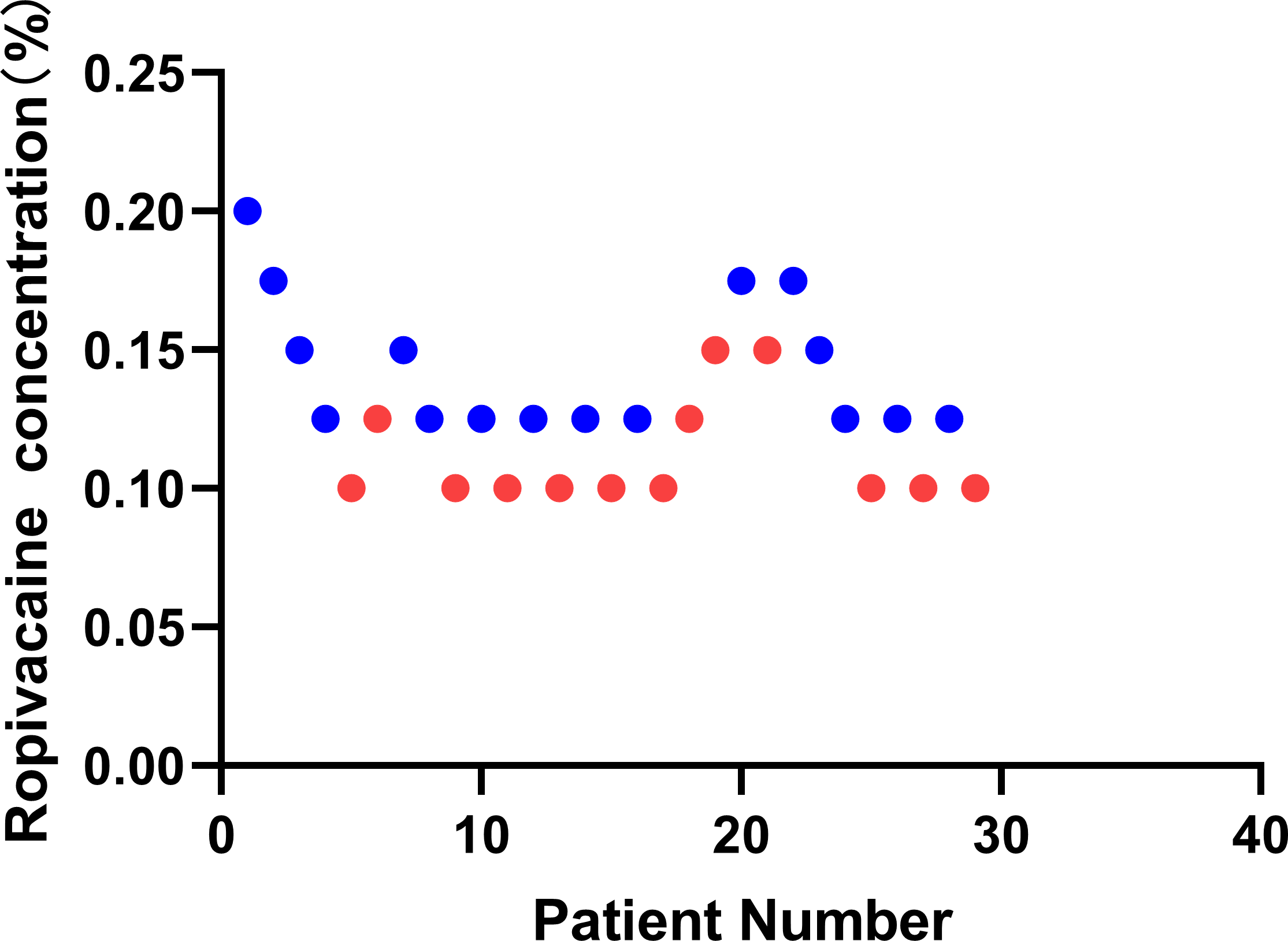
Background: This study aimed to determine the median effective analgesic concentration of 10mL ropivacaine in interscalene brachial plexus block for postoperative anesthesia in 50% of the patients (EC50). Method: This study was conducted on 30 patients with ASA grade I or II, who are planning to undergo proximal humerus fracture operation. A concentration of 10mL ropivacaine administered for the Interscalene brachial plexus was determined using the up-and-down sequential. The initial concentration of ropivacaine in the first patient to receive interscalene brachial plexus block(ISBPB) was 0.3%, After a successful or unsuccessful postoperative analgesia, the concentration of local anesthetic was decreased or increased, respectively, by 0.05% in the next patient. We defined successful postoperative analgesia as VAS score below 4 at rest within initial 8 hours after ISBPB. The analytic techniques of linear, linear-logarithmic, exponential regressions and centered isotonic regression were used to determine the EC50 of ropivacaine and the residual standard errors were calculated for the comparison of “goodness of fit” among the different models. Results: The concentration of ropivacaine administered ranged from 0.1% to 0.35%. The EC50 (95% confidence interval) from 4 different statistical approaches (linear, linear-logarithmic, exponential regressions and centred isotonic regression) were 0.222% (0.198%, 0.335%), 0.233% (0.215%, 0.453%), 0.223% (0.202%, 0.436%), and 0.232%, respectively. Among all of the 4 models, the linear regression had the least residual standard error (0.1676). Conclusion: The EC50 derived from four statistical models for 10ml ropivacaine in ultrasound-guided interscalene brachial plexus block for postoperative analgesia was distributed in a narrow range of 0.222%–0.233%.